


Deconstructing the LIES: Refuting the propaganda for maternal Tdap vaccination
Shocking facts .. but true.

BS”D
Many people have contacted me asking for my thoughts on an unfortunate vaccine propaganda article recently published by a government mouthpiece:
That article hysterically promotes vaccines for two different diseases using unconfirmed stories and lots of fear mongering. In fact, while the doctor is at it, she throws in how “grateful” we have to be for the covid vaccine, too!
I will focus here on deconstructing the falsities surrounding maternal Tdap vaccination, the article’s first topic, as YWN quotes the doctor’s implication that a baby died of pertussis because his or her mother did not get the pregnancy Tdap booster. There is zero factual data included on how well such shots actually work, what risks they have, and what the balance is of pertussis risk vs. vaccine risk.
Wait - don’t you know that you’re obligated to start getting every new vaccine for pregnancy that the vaccine makers decree, without asking any forbidden questions, or you will be an anti-vaxxer?
If you’re a parent in your late thirties or in your forties, you might remember that no one was suggesting you get a Tdap vaccine in pregnancy fifteen years ago. The recommendation is really quite new:
But now that vaccine manufacturers have carved out a lucrative new market, and gotten the FDA and CDC to rubber-stamp this injection in pregnant women, shame on you if you don’t let them shoot you up in your next pregnancy. You’re endangering your baby! If he or she dies of whooping cough, it’ll be on your head, you ignorant anti-vaxxer!
That’s what the shameless government mouthpiece in my community is broadcasting.
What’s the REAL story?
We always want to weigh the risks and benefits of every decision in life, especially ones that can be life-or-death. So:
•What are the chances that a newborn will die of whooping cough?
•Will the vaccine reduce that risk, and if so, by how much?
•What other risks will the Tdap vaccine expose the mother and baby to?
•In the final analysis, does Tdap vaccination in pregnancy decrease or increase the chance of the baby’s death, from any cause?
Look for the answers to these questions as you read through this article, and expect to be surprised.
Fast stats:
How many babies die each year of whooping cough in the US?
The CDC claims that since 2010, up to 20 babies have died each year.
I wish we had a more exact figure, and I am unsure whether their diagnostics were accurate (more on that later), but for now let’s run these numbers.
I picked 2015 as an in-between year since 2010, for population data:
I divided the 3,978,000 births/year by the 20 “whooping cough” baby deaths/year to see what the odds are that a baby in the US will die of whooping cough, and I found that there’s a 1 in 198,900 chance that a baby born in the US will die of whooping cough.
Being that the risk of baby’s whooping cough death is so remote, parents had better question: “Is there a risk to the getting the whooping cough vaccine?”
And it turns out that there is!
How safe is the Tdap vaccine in pregnancy, anyway?
Actually, not very safe.
I found these three journal articles:
•https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5546155/
Keep in mind that in this study, they looked at insurance claims for live births, so they will miss miscarriages and stillbirths.
This study found an increased rate of postpartum maternal hemorrhage in women who received the Tdap in pregnancy. Twelve vaccinated mothers also developed encephalopathy after delivery. Most concerning to the baby’s welfare, women vaccinated with Tdap during pregnancy had an increase in a potentially deadly-to-the-baby infection of the placenta and amniotic fluid, called chorioamnionitis. In fact, this was the second study to find an increase in chorioamnionitis and postpartum hemorrhage among Tdap vaccinated mothers.
How serious is chorioamnionitis?
Well, it’s an infection surrounding the baby, so it’s very serious. It may necessitate the baby’s immediate birth, even if the baby is very preterm. The baby may be left with permanent complications from prematurity and/or from the infection.
I’m having difficulty understanding why it would be logical or appropriate to expose a mother and baby to the risks of chorioamnionitis from the Tdap vaccine in pregnancy, in order to offer some protection against the 1 in 198,900 chance that the baby will die of whooping cough.
•https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8903913/ This article reports on the findings from the vaccine maker’s pregnancy registry. Hidden towards the end, we discover that 6.3% of women in the registry who received Tdap in pregnancy reported a serious adverse event.
•https://www.sciencedirect.com/science/article/pii/S0264410X23004577 “Tdap vaccination during pregnancy and risk of chorioamnionitis and related infant outcomes” This is the first study that found the increased risk of chorioamnionitis. They constructed the study in a way that they only looked at live births, in order to avoid showing the babies who were lost to miscarriage or stillbirth.
(Note - when reading journal articles, it is most important to remember the many tricks used in studies in order to conceal and minimize negative outcomes. For example, those who died or experienced severe complications are often removed or “lost to follow up.” A small sample will be left, in whom the intervention may appear not to have caused unusual effects. When a danger signal is nevertheless detected, the article will nevertheless summarize by saying the study intervention “appears safe,” (“forget the negative effects we just told you about!”) or that “more study is needed.” There are many other ways that studies and clinical trials are manipulated as well, such as by comparing two groups who are both exposed harmful substances.)
After seeing the grave risks to mother and baby of the Tdap vaccine as illustrated here, you should also know that it does not even offer the baby complete protection from whooping cough. In fact, the CDC does not even try to make such a claim.
Remember, there’s no benefit in dying from chorioamnionitis complications while being somewhat protected from whooping cough. It’s overall mortality and morbidity that's important. There have been no long-term studies of women who received vaccines during pregnancy. Nor have there been any long-term studies of babies born to mothers who received vaccines during pregnancy.
Who said the baby in the YWN story actually had whooping cough?
It is very likely that the baby who is reported to have “died of whooping cough” did not even have whooping cough at all. A diagnosis from a PCR test is meaningless, and many other common respiratory ailments completely mimic whooping cough, as this NYT (!) article from 2007 so helpfully explains: https://www.nytimes.com/2007/01/22/health/22whoop.html
Excerpts:
Faith in Quick Test Leads to Epidemic That Wasn’t
The New York Times
By Gina Kolata
Jan. 22, 2007
Dr. Brooke Herndon, an internist at Dartmouth-Hitchcock Medical Center, could not stop coughing. For two weeks starting in mid-April last year, she coughed, seemingly nonstop, followed by another week when she coughed sporadically, annoying, she said, everyone who worked with her.
Before long, Dr. Kathryn Kirkland, an infectious disease specialist at Dartmouth, had a chilling thought: Could she be seeing the start of a whooping cough epidemic? By late April, other health care workers at the hospital were coughing, and severe, intractable coughing is a whooping cough hallmark. And if it was whooping cough, the epidemic had to be contained immediately because the disease could be deadly to babies in the hospital and could lead to pneumonia in the frail and vulnerable adult patients there.
It was the start of a bizarre episode at the medical center: the story of the epidemic that wasn’t.
For months, nearly everyone involved thought the medical center had had a huge whooping cough outbreak, with extensive ramifications. Nearly 1,000 health care workers at the hospital in Lebanon, N.H., were given a preliminary test and furloughed from work until their results were in; 142 people, including Dr. Herndon, were told they appeared to have the disease; and thousands were given antibiotics and a vaccine for protection. Hospital beds were taken out of commission, including some in intensive care.
Then, about eight months later, health care workers were dumbfounded to receive an e-mail message from the hospital administration informing them that the whole thing was a false alarm.
Not a single case of whooping cough was confirmed with the definitive test, growing the bacterium, Bordetella pertussis, in the laboratory. Instead, it appears the health care workers probably were afflicted with ordinary respiratory diseases like the common cold.
Now, as they look back on the episode, epidemiologists and infectious disease specialists say the problem was that they placed too much faith in a quick and highly sensitive molecular test that led them astray.
Yes, the faulty test was the PCR test. The NYT would never publish this article today. In fact, while it used to be free, they’ve now put it behind a paywall.
There are no national data on pseudo-epidemics caused by an overreliance on such molecular tests, said Dr. Trish M. Perl, an epidemiologist at Johns Hopkins and past president of the Society of Health Care Epidemiologists of America. But, she said, pseudo-epidemics happen all the time. The Dartmouth case may have been one the largest, but it was by no means an exception, she said.
There was a similar whooping cough scare at Children’s Hospital in Boston last fall that involved 36 adults and 2 children. Definitive tests, though, did not find pertussis.
“It’s a problem; we know it’s a problem,” Dr. Perl said. “My guess is that what happened at Dartmouth is going to become more common.”
It certainly has.
“You’re in a little bit of no man’s land,” with the new molecular tests, said Dr. Mark Perkins, an infectious disease specialist and chief scientific officer at the Foundation for Innovative New Diagnostics, a nonprofit foundation supported by the Bill and Melinda Gates Foundation. “All bets are off on exact performance.”
Of course, that leads to the question of why rely on them at all. “At face value, obviously they shouldn’t be doing it,” Dr. Perl said. But, she said, often when answers are needed and an organism like the pertussis bacterium is finicky and hard to grow in a laboratory, “you don’t have great options.”
Waiting to see if the bacteria grow can take weeks, but the quick molecular test can be wrong. “It’s almost like you’re trying to pick the least of two evils,” Dr. Perl said.
At Dartmouth the decision was to use a test, P.C.R., for polymerase chain reaction. It is a molecular test that, until recently, was confined to molecular biology laboratories.
“That’s kind of what’s happening,” said Dr. Kathryn Edwards, an infectious disease specialist and professor of pediatrics at Vanderbilt University. “That’s the reality out there. We are trying to figure out how to use methods that have been the purview of bench scientists.”
The Dartmouth whooping cough story shows what can ensue.
To say the episode was disruptive was an understatement, said Dr. Elizabeth Talbot, deputy state epidemiologist for the New Hampshire Department of Health and Human Services.
“You cannot imagine,” Dr. Talbot said. “I had a feeling at the time that this gave us a shadow of a hint of what it might be like during a pandemic flu epidemic.”
Yet, epidemiologists say, one of the most troubling aspects of the pseudo-epidemic is that all the decisions seemed so sensible at the time.
Hmm..
The disease got its name from its most salient feature: Patients may cough and cough and cough until they have to gasp for breath, making a sound like a whoop. The coughing can last so long that one of the common names for whooping cough was the 100-day cough, Dr. Talbot said.
But neither coughing long and hard nor even whooping is unique to pertussis infections, and many people with whooping cough have symptoms that like those of common cold: a runny nose or an ordinary cough.
“Almost everything about the clinical presentation of pertussis, especially early pertussis, is not very specific,” Dr. Kirkland said.
That was the first problem in deciding whether there was an epidemic at Dartmouth.
The second was with P.C.R., the quick test to diagnose the disease, Dr. Kretsinger said.
With pertussis, she said, “there are probably 100 different P.C.R. protocols and methods being used throughout the country,” and it is unclear how often any of them are accurate. “We have had a number of outbreaks where we believe that despite the presence of P.C.R.-positive results, the disease was not pertussis,” Dr. Kretsinger added.
At Dartmouth, when the first suspect pertussis cases emerged and the P.C.R. test showed pertussis, doctors believed it. The results seem completely consistent with the patients’ symptoms.
“That’s how the whole thing got started,” Dr. Kirkland said. Then the doctors decided to test people who did not have severe coughing.
“Because we had cases we thought were pertussis and because we had vulnerable patients at the hospital, we lowered our threshold,” she said. Anyone who had a cough got a P.C.R. test, and so did anyone with a runny nose who worked with high-risk patients like infants.
“That’s how we ended up with 134 suspect cases,” Dr. Kirkland said. And that, she added, was why 1,445 health care workers ended up taking antibiotics and 4,524 health care workers at the hospital, or 72 percent of all the health care workers there, were immunized against whooping cough in a matter of days.
“If we had stopped there, I think we all would have agreed that we had had an outbreak of pertussis and that we had controlled it,” Dr. Kirkland said.
But epidemiologists at the hospital and working for the States of New Hampshire and Vermont decided to take extra steps to confirm that what they were seeing really was pertussis.
The Dartmouth doctors sent samples from 27 patients they thought had pertussis to the state health departments and the Centers for Disease Control. There, scientists tried to grow the bacteria, a process that can take weeks. Finally, they had their answer: There was no pertussis in any of the samples.
This obviously leads us to ask, how was the unfortunate baby in Israel who is supposed to have “died of whooping cough” diagnosed? He or she just died, so the diagnosis was certainly not with the reliable sort of test, in which the bacteria can take weeks to grow in the laboratory.
And of course now the question is also, how are the “up to 20 babies per year” that the CDC claims die of whooping cough, actually diagnosed? Is it on the basis of the PCR tests, which caused the false “epidemic” in Dartmouth?
Who said the baby died OF whooping cough, rather than negligence (or worse?)
This sounds like a horror movie, but it’s real:
It was well-known in Israel during covid that people who were unvaccinated were in extreme danger of being killed, were they to go to the hospital. I don’t know who the evil individuals are, but there were murderers making sure that whoever they could get their hands on did not make it out alive. Surely their goal was to raise the “covid” death count to promote fear, so that the covid vaccine would be accepted by the population.
Now that so many have lost trust in the system and childhood vaccine uptake has plummeted, the Health Ministry has been attempting one fear-mongering scam after another.
In one of their first post-covid fakes, two little girls in Jerusalem supposedly had polio. This was going to be big, scary news and whip the scores of new anti-vaxxer parents back in shape! So, I spoke to both of the children’s mothers. The first mother thinks her daughter indeed had polio. The catch? She was infected by her preschool classmate, who had just gotten the live vaccine, which sheds.
Next: The second Jerusalem “polio case” was an outright lie. The girl was healthy, but had ongoing digestive issues due to poor diet. The mother took her to the pediatrician for a workup, and got a call a couple weeks later that the test results all showed a clean bill of health. A while later, the pediatrician started calling her every day, asking about her children’s vaccination status (vaccines are given at health clinics, and pediatricians don’t have access to those records.) This mother likes to delay childhood shots, and she was reluctant to admit that. After a week of incessant pestering, though, she finally confessed that her kids were behind schedule. Almost as soon as she admitted that, she got a call from the Health Ministry “your child has polio, you must immediately bring her and your other young children to be vaccinated.” When the stunned mom questioned the safety of vaccinating during an illness, she was met with anger. She unsuspectingly took her children to the clinic where they received both the inactivated and the live polio vaccines. It was only when the Health Ministry called her back and said they wanted to come collect stool samples from all her children, that she smelled something rotten, and got a lawyer. When the lawyer requested the lab results that showed the child had polio, the government dropped the case. Their cunning plan had been to “find” polio in the stool of all the children - and they would have found it, because the children had recently received the live polio vaccine, courtesy of the Health Ministry.
The next year, media reported a “polio outbreak” in Safed. The only problem is, I happen to have relatives there, and it’s a small town. So I found out that the kids who supposedly had polio, were actually polio-vaccinated kids.
The moral of the story: The Health Ministry, and their doctor pawns and mouthpieces, will (just like the CDC and FDA) do whatever it takes to get vaccination rates up. Truth and morality mean nothing to them. Therefore, all reports similar to the YWN article linked here are much more likely to be false, than to be true.
Why weren’t the effective treatments for whooping cough given to the baby? (Why isn’t there education provided to parents and medical practitioners about proper whooping cough treatment?)
The idea that our bodies are absolutely helpless against evil pathogens until a modern-invented vaccine is administered is a fallacy.
Yes, many children used to die of infectious diseases, when they were malnourished and lacked adequate sanitation. We don’t live in those times anymore, and we don’t need to keep that fear alive. Whooping cough mortality had already dropped 92% before the pertussis vaccine came to be in widespread use in the 1940’s. It is not the whooping cough vaccine that stopped the vast majority of whooping cough deaths.
G-d has created treatments for everything, including whooping cough. As the Torah teaches, He created the “cure before the disease.”
From the Childhood Vax Library Telegram group: https://t.me/+4ZWCtSBFRX45MmVk
Way back in the 1930s, vitamin C / ascorbic acid was being recognized as an effective way to treat whooping cough - to neutralize the pertussis toxin and reduce the length and severity of the infection.
But guess what else was being developed at that time? The first pertussis vaccine.
When a vaccine is introduced, there is little to no attention or funding given to the development of alternative treatment options. This would undermine the vaccine industry. Therefore, there has not been any more research on this, since then: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1562195/
It is a crime that “modern medicine” suppresses cures for the sake of profit and control.
Parents need to know that Dr. Suzanne Humphries MD has a very effective Vitamin C protocol for whooping cough which can be used on the youngest infants to get them through the illness safely at home: https://drsuzanne.net/2017/10/sodium-ascorbate-vitamin-c-treatment-of-whooping-cough-suzanne-humphries-md/
Additionally, nebulizing regularly with properly diluted hydrogen peroxide is a tried-and-true aid to get through whooping cough rapidly and with reduced symptoms. Please be sure to receive expert guidance.
How effective is the DTaP/Tdap vaccine, anyway?
I quote portions of MD Suzanne Humphries’ website: https://drsuzanne.net/2017/10/sodium-ascorbate-vitamin-c-treatment-of-whooping-cough-suzanne-humphries-md/
“If the B. pertussis vaccine was safe and effective, it may have been worth using. However, the B. pertussis vaccine is provably one of the most ineffective. Its many disadvantages which lend dubious, fleeting protection to the individual, results in numerous doses and boosters from cradle to grave. In fact, the more whooping cough vaccines a person receives, the less effective they become.[1] Diavatopoulis has even compared the acellular vaccine that is used today, to allergy shots, because the cellular immune system responds less and less after successive doses in those who have been primed with acellular vaccines.
“Conversely one episode of natural whooping cough renders the recovered person immune far longer than any series of vaccines will.
“A 2010 study suggested that natural immunity to whooping cough lasts at least 30 years[2], whereas the immunity from a vaccine lasts three years at most.[3]
“If you think that a vaccinated person cannot get whooping cough, in the most severe manner, think again. Most babies over the age of 6 months who get whooping cough are fully and “appropriately” vaccinated. In 2012, a new peer reviewed document from professor of infectious diseases, Dr Maxwell Witt of Kaiser Permanente in California showed that B. pertussis runs rampant in fully vaccinated child populations.
“Our data suggests that the current schedule of acellular pertussis vaccine doses is insufficient to prevent outbreaks of pertussis. We noted a markedly increased rate of disease from age 8 through 12 . . . . Acellular vaccines have not been studied for clinical efficacy in north America and no studies exist on long term.”[4]
“Quite impressive, right? Table 1 at the end of Dr Witt’s document shows the percent of cases in the vaccinated, and it as follows: 86% age 2-7, 86% age 8-12, 62% age 13-18, 81% age 2-18. So now you know who gets more B. pertussis. It is not the unvaccinated. He even says, in the introduction:
“Our unvaccinated and under-vaccinated population did not appear to contribute significantly to the increased rate of clinical pertussis. Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group.”
“The rate of infections in the vaccinated is huge. Look at this chart prepared by the California Department of Public Health, Immunization Branch.
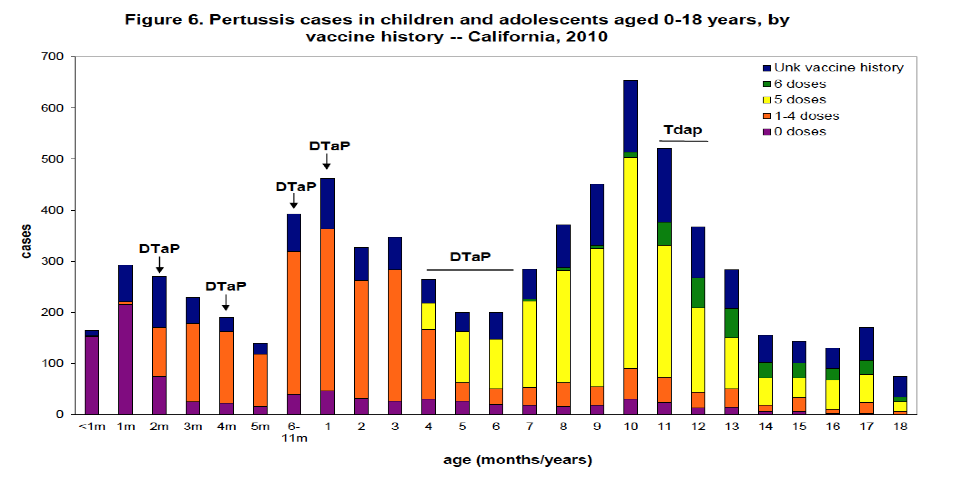
“The above chart was last printed in the California department of public health pertussis report[5], November 10, 2011. Thereafter, the report on cases by vaccine history stopped. In fact, word searching for ‘vaccine’ brings up no data in the recent reports. It just says to give the vaccine in infancy and pregnancy.
Personal protection: Who wins out?
“Vaccinated babies, children, and adults are not able to mount the comprehensive bronchial and cellular immunity that a non-vaccinated person naturally develops in the course of the disease.[6] Why? Because the vaccine primes the body to fight B. pertussis toxin and sometimes a couple of other bacterial antigens, in the blood, but does not provide protection at the lung interface where the real-life battle occurs. The ineffective immunity “learned” from the vaccine series (referred to by Dr. James Cherry as “original antigenic sin”)[7], is the same way the body will respond to a subsequent natural exposure.
“The learned immune response to an acellular vaccine results in numerous differences compared with the normal response mounted to a natural infection. Some of the key differences in vaccinated people are:
Antibody preferentially made in the blood rather than the lung interface.
IgG antibody rather than IgA antibody.
A relatively different and ineffective antibody because the vaccine antigens are not the same shape as the real life antigens.[8]
A relative, progressive loss of protection with each vaccine dose, because the T cell response is similar to what allergy injections do.[9]
Far lower complement-mediated killing of bacteria.
Suboptimal inflammatory responses resulting in impaired lung clearance of bacteria.
Impaired phagocytosis.
“It is well known that never-vaccinated B. pertussis disease-convalesced children, develop important immune responses that the vaccinated do not[10]. Vaccine developers have attempted to compensate for this phenomenon by creating vaccines with multiple antigens. The point they miss, is that it is only front line, innate, and naturally acquired complex-cellular and bronchial responses, which give the full protection. It has been shown that response to B. pertussis toxin[11] and adenylate cyclase toxin[12]is far more robust in the unvaccinated, than the vaccinated. Because of this, naturally immune people, upon re-exposure, will clear bacteria far more rapidly than the vaccinated will. There is an enormous difference between broad, long-lasting immunity from the normal disease, and limited antibody development and short-term pseudo-immunity from the vaccine.”
(End quotes.)
Note: In regards to “cocooning,” in which all of a new baby’s close contacts are supposed to be freshly vaccinated against pertussis, a landmark study published in 2013 showed that this recommendation is illogical and could even be harmful, as the Tdap shot does NOT prevent whooping cough transmission. Vaccinated people can be become infected and be carriers without realizing it.
Childhood Vax Resource Library:
The National Academy of Science of the United States of America did a Pertussis baboon study showing transmission after vaccination: http://www.pnas.org/content/111/2/787.full
The study in infant baboons showed that the pertussis vaccine does not eliminate transmission of B. pertussis whooping cough. The baboon study suggests that if you’re recently vaccinated against whooping cough and then are exposed to B. pertussis, you may not get classic symptoms of the disease but could temporarily become an asymptomatic carrier.
Parents: Please read Turtles All the Way Down: Vaccine Science and Myth (pages 321-327), for a deeper understanding of what this very important baboon study means to the entire DTaP/Tdap vaccination program.
How safe dangerous is the DTaP/Tdap vaccine in general?
Most “Sudden Infant Death” happens after a “well visit,” with the DTaP vaccine being the shot most often resulting in tragedy.
From Childhood Vax Resource Library:
Dr. Viera Scheibner, a research scientist who has conducted many studies of SIDS, measured episodes of apnea (breathing cessation) and hypopnea (abnormally shallow breathing) in infants both before and after they received DTP vaccination.
The information was gathered using a breathing monitor that generates computer printouts of breathing activity. Dr. Scheibner noted a significant increase in the incidence of both apnea and hypopnea after vaccination, and that these episodes continued for several months. Her findings led her to conclude that "vaccination is the single most prevalent and most preventable cause of infant deaths." Read more on Dr. Scheibner's story here:
Getting back to the main topic of our article - maternal Tdap vaccination - we must ask: How could it possibly be safe to give a shot that is associated with a significant increase in baby death … to unborn babies, who receive it through the placenta, when the mother gets vaccinated in pregnancy?
I wrote at length about the dangers of DTap for babies and children in this recent article: www://truth613.substack.com/p/whats-really-in-childhood-vaccines
Parents, don’t let yourselves be bullied. Do real, unbiased research and then stand strong in what you will KNOW is the safer option for your baby.
Your doctor is unfortunately not an “expert” just because he or she is a “doctor.”
I believe that by this point you will agree that the correct title for an article about the Tdap and DTaP vaccines should actually be: “Why do parents who love their children expose them to deadly vaccines?”
This article was reviewed by Lynn Z. M.D. and James Thorp M.D. OB-GYN. Please see Lynn Z.’s message:
Message from Lynn Z. MD
Tdap Vaccines in Pregnancy by Lynn Z. M.D.
1/198,000 unvaccinated infants die each year from whooping cough, a.k.a. pertussis. This is assuming the testing is accurate – which it is not because the PCR test is used. The PCR test tests for only a small portion of the isolated DNA and by the lab’s own admission, it is highly inaccurate, resulting is a lot of false positives, which in another words means that when the results say you have pertussis, you actually don’t have pertussis.
That comes to 0.00005% of infants who die of what is called whooping cough, given that this is an overestimation because of the testing used to make the diagnosis.
https://www.cdph.ca.gov/Programs/CID/DCDC/CDPH%20Document%20Library/Immunization/PertussisLabTesting.pdf
Of those pregnant women who get the vaccine, 6.3% have a serious adverse event. Examples of serious adverse events are encephalopathy, chorioamnionitis, and death.
0.000005% (nonvaccinated) vs. 6.3% (vaccinated) with unfortunate outcomes….. Hmmmm.
Common sense should prevail:
It is only from innate immunity that you get full protection. Innate immunity is when the lining of the lung is exposed to the antigen and you develop immunity to the entire “genre” of the virus, rather than one strain. Adaptive immunity is when you get a vaccine and develop protection to that particular strain which leaves you actually more exposed to all of the other strains. Plus, adaptive immunity (to that particular strain) is temporary. Innate immunity (to the entire “genre”) lasts decades, and for some, a lifetime.
The fetus who “receives” the vaccine because the mother is vaccinated, or the infant after birth who receives the vaccine is at risk of all sorts of dangerous effects on the brain because the blood brain barrier is porous at birth and does not fully mature and become a functioning barrier until six months of age – meaning that whatever is injected into the bloodstream, which includes the adjuvant metals that are placed into the vaccines goes directly into the brain. (Here lies the birthchild of all sorts of neurological disorders such as autism.)
The immune system is not fully developed until age two, therefore receiving any vaccine before this age will decrease the ability of the child to develop their natural and robust innate immunity.
Bottom line:
There is a higher risk of morbidity and mortality including neuroinflammatory diseases if a child is vaccinated before six months. There is a higher risk of being susceptible to all infectious diseases if a child is vaccinated before two years. You have been duly informed. Make the best decision you can for yourself and your unborn child.
To help me continue my work, you may make a one-time gift here: https://ko-fi.com/truth613
As someone who has been fighting the insanity of these vaccines, especially in the context of pregnacy it warms my heart to see how many are now in the fight. I only wish you were there with me a quarter of century ago. It was just a very small handful of us.
Excellent article. The shaming of the mother of the dead child is unforgivable, but what I have come to expect. Perhaps someone will reach out to her with the truth so she won't be carrying such guilt. Now if she got the shot and her child died from chorioamnionitis- you wouldn't hear anything from the medical est. or their mouth pieces. I doubt if it was whooping cough- according to the CDC, (center for deception, control and propaganda) whooping cough is so contagious that 8-10 nonimmune people will be infected when exposed to the disease. Did her mother, father, care takers come down with it? I wouldn't rule out the child had a reaction to a childhood vaccine. Since it makes sense to question the diagnosis of whooping cough using pcr test and of the 20 or so deaths assigned to it in the US each year- one should also question pre-vaccine cases that created the basis for this vaccine.