


Part 1: Withholding treatment is MURDER
How can you trust a murderer?

BS”D
Sometimes, I am asked “How do you know which side is the truth?”
Now, when you read enough, you just know. You see one side that searches for truth and brings real research and data. That’s the side that is suppressed and censored. Those are the people who have to be brave and risk - or actually lose - careers in order to get their findings out.
You see another side who brings you sweet-sounding, reassuring little bytes but no real science. When they do bring “studies”, the studies are deeply flawed and the authors have severe conflicts of interest. This is the side who is paid off to promote the narrative and hasn’t done real research. The side that’s doing the censoring.
But let’s say someone hasn’t done that much reading, so they haven’t noticed this yet. And they’re asking how you know which side is right.
So here’s an excellent place to start realizing the truth from: the suppression of effective treatments for covid, from Day 1. Once you realize that this was done, very consciously and systematically, you realize that you cannot trust whoever did that with your life. And, they’re the same people pushing the you-know-what. So it quickly becomes clear that something is wrong.
On that note, here, G-d willing, I want to bring you some astounding pieces of the story about the suppression of ivermectin, one of the most wondrous and safe drugs in a physician’s arsenal.
Back in April, I wrote about the TOGETHER trial, a huge trial of covid treatments in Brazil which was highly problematic, and a perfect example of a study rife with conflicts of interest and flaws, as I mentioned above. It’s obvious to whoever looks closely that the trial was rigged to make ivermectin appear to have as little efficacy as possible.
Imagine that you have a financial interest in the vaccines, and that widespread knowledge of safe and effective treatments would render covid not-very-scary-anymore and ruin demand for your brand-new genetic therapy injection. What better way to take down the competition than to straight-facedly pretend to be running a trial to see which early treatments will work well, and of course do your best to make sure that none of them come out looking too good? That’s the summary of what happened.
Here’s my April 1 article and follow up podcast update:

One of the biggest problems in the trial was the widespread use of ivermectin in Brazil, since it’s available over the counter, and was especially being widely used at the time the trial was taking place. This means that much of the “placebo” group was undoubtedly on ivermectin too, so of course, much less difference will be seen between “treatment” and “placebo” group (false conclusion, treatment not significantly helpful.)
Here in Part 1, I want to bring you new, fascinating information about this “placebo group” problem. (Part 2 will show the amazing, documented success story of the vast Indian state of Uttar Pradesh totally crushing covid by its state government promoting and distributing ivermectin - and how mainstream media continues to ignore this.)
Did the Placebo Group in the TOGETHER Trial Take Ivermectin?
Alexandros Marinos
Aug 7
The problem of community use of ivermectin in Brazil at the time the TOGETHER trial was trialing high-dose ivermectin has been discussed to no end. And yet, I don’t think I’ve ever brought all the collected evidence together.
This article aims to be a straightforward aggregation of all the clues we have, hopefully pointing the way to an answer.
The most helpful way I know to answer the question is by breaking it up into smaller ones. First, was community use prevalent? And second, did the trial successfully isolate itself from the effects of any use in the community?
Was Community Use of Ivermectin a Problem?
In late 2020, a curious article from NatureMagazine made the rounds:

Its chief concern? That people might take “unchecked use” of ivermectin, an “unproven COVID treatment,” therefore local studies might struggle to recruit patients:
Some early studies in cells and humans hinted that the drug has antiviral properties, but since then, clinical trials in Latin America have struggled to recruit participants because so many are already taking it.
“Of about 10 people who come, I’d say 8 have taken ivermectin and cannot participate in the study,” says Patricia García, a global-health researcher at Cayetano Heredia University in Lima and a former health minister for Peru who is running one of the 40 clinical trials worldwide that are currently testing the drug. “This has been an odyssey.”
Forgive me while I wipe my tears as regular people infected with COVID—people who had zero treatment options available to them in 2020—dared use a cheap over-the-counter medication with a safety record stretching back many decades, submitting a few researchers to “an odyssey.” If you have to tell people to wait around for a year— dying while you make sure the thing with no downside they can readily take will definitely help them or not (after they have recovered or died)—maybe it’s your science that needs to change, not people’s behaviour.
This kind of ivory tower thinking really makes my blood boil, but I digress.
[Editor’s note: Right about now is when Alexandros is making a superhuman effort not to go off on a tangent about “unchecked use” of “unproven measures” such as “lockdowns,” “school closures,” and “masking 2-year olds.”]
Back to Nature:
Still, researchers might never have sufficient data to justify ivermectin’s use if its widespread administration continues in Latin America. The drug’s popularity “practically cancels” the possibility of carrying out phase III clinical trials, which require thousands of participants — some of whom would be part of a control group and therefore couldn’t receive the drug — to firmly establish safety and efficacy, says Krolewiecki.
As unchecked use of ivermectin grows, he says, “the more difficult it will be to collect the evidence that regulatory agencies need, that we would like to have, and that will get us closer to identifying the real role of this drug”.
What the article says, in brief, is that if a large portion of people in a region are taking ivermectin, it becomes very difficult to create a representative control group for a randomized controlled trial (RCT), since those groups have to not be taking the drug for the trial to have validity.
This matches my own experience: I once asked a clinical researcher from a Latin American country how much it would cost to set up a proper ivermectin RCT in his country. His response stumped me. He said there was no way to form a control group for an RCT since so many people were already on ivermectin there.
Even though the Nature article was published in October 2020—making the case that running large-scale RCTs in Latin America without distorting the results due to community use would be incredibly difficult—the TOGETHER trial started doing just that—only a few months later—in January 2021. The trial started with an incredibly low dose, and had to restart its ivermectin arm, which it did on March 23rd.
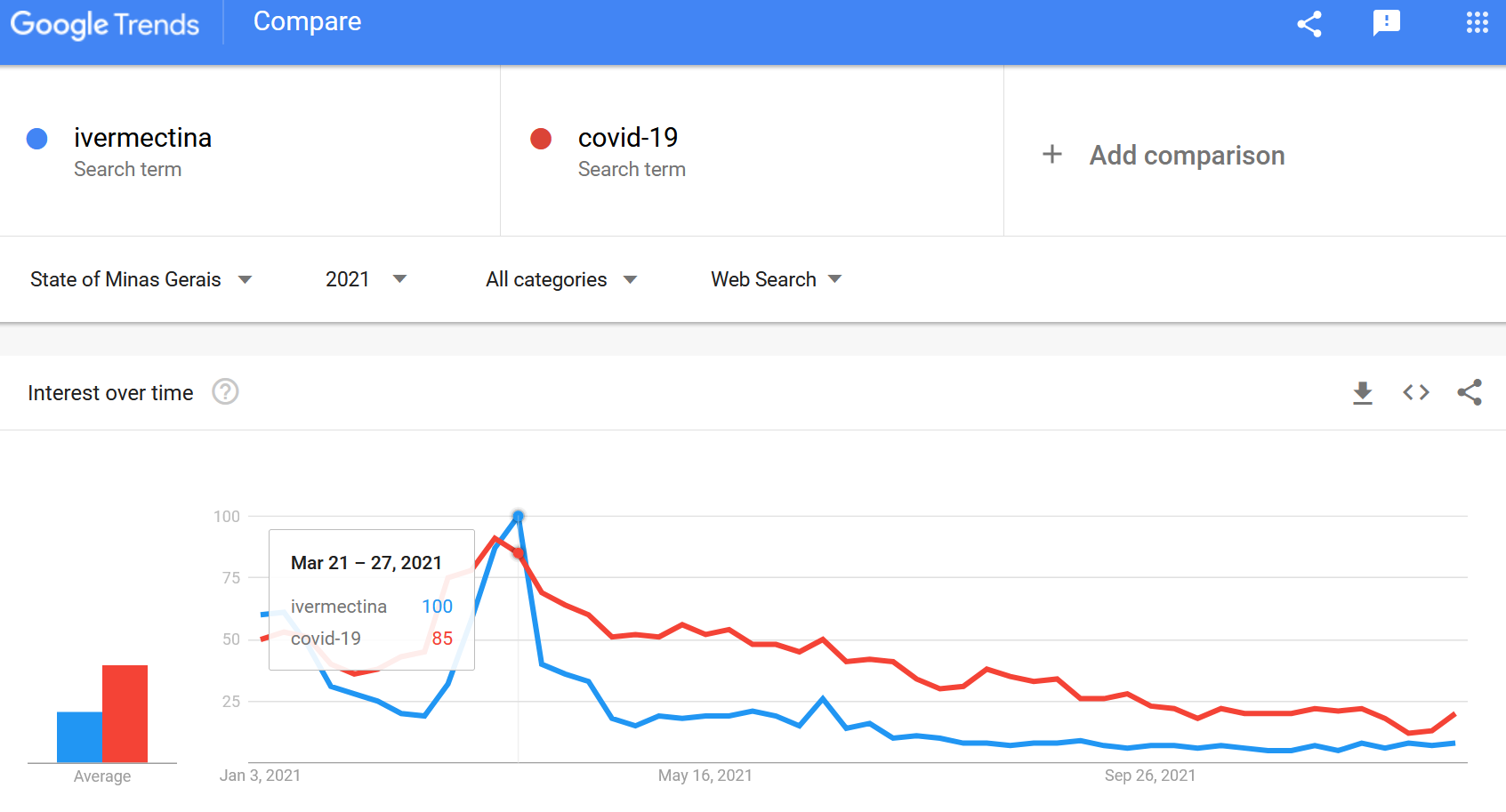
If we have a look at Google Trends, we find that interest in ivermectin in the state that the TOGETHER trial took place was off the charts, exactly at the time the high-dose ivermectin arm started, even exceeding search traffic to “covid-19” for a few days.
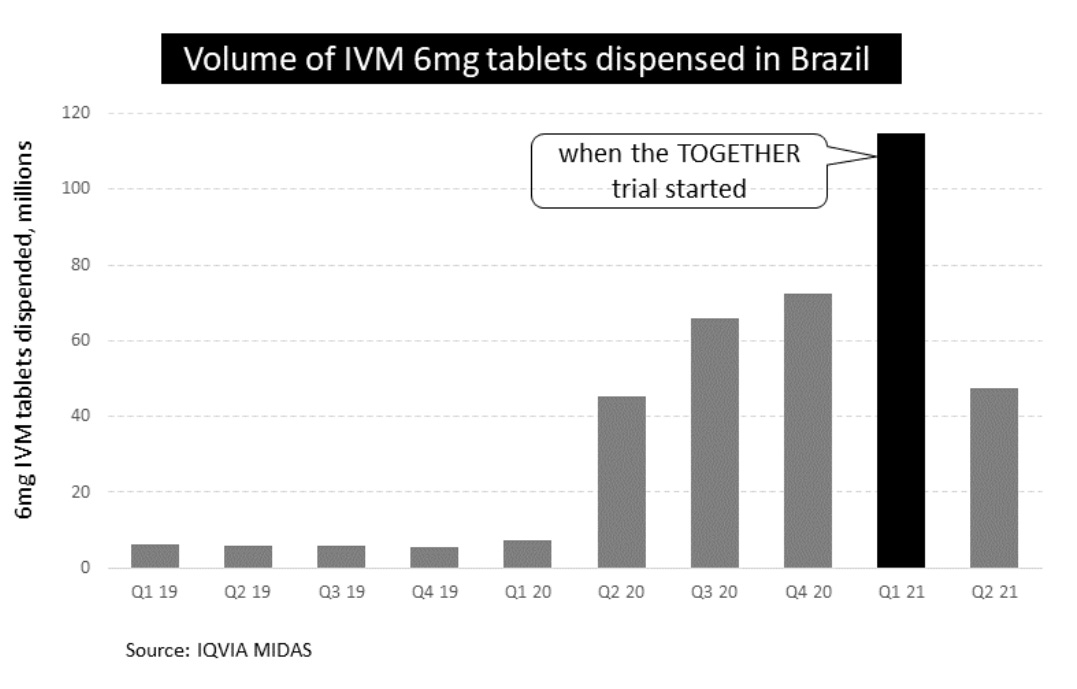
Sales were also through the roof around that time. We can see this from commercially available data:
Strangely, the principal investigator, Dr. Ed Mills, had a puzzling response to a question about this issue:
At the time we did our study, IVM was not particularly popular for use in Minas Gerais. Even if some patients did access IVM, the fact that it is blinded should still maintain balance.
What could “the fact that it is blinded should still maintain balance.” mean? The only thing I can imagine it meaning is that if the patients who were taking ivermectin are equally distributed across treatment and control arms, the benefit should be equal to both arms, and therefore not impactful to the final result.
This, of course would imply that Dr. Mills was aware that increasing the dose that the patients in the treatment arm were taking would yield additional benefit in a linear fashion, similar to the benefit the control group would get from the out-of-trial usage. But if that was the case, why not give patients more of the drug in the first place?
The general sentiment expressed however, that ivermectin was not in broad use, matches an earlier comment attributed to Dr. Mills.

If this is indeed his response, it's puzzling, as low community use should make it easy to add to the exclusion criteria, for avoidance of doubt.
These statements fly in the face of what was written by the investigators (including Mills, one imagines) in the NEJM publicationreporting on the trial, which clearly says:
Ivermectin has been used off-label widely since the original in vitro study by Caly et al. describing ivermectin activity against SARS-CoV-2,22 and in Brazil, in particular, the use of ivermectin for the treatment of Covid-19 has been widely promoted.
Not only that, but Mills’ argument proves too much. If “the fact that it is blinded” makes this not an issue, why have exclusion criteria at all?
Reports at the time from the local pressdefinitely indicate that Mills’ statements are not right:

Given that the statement by Ed Mills is in conflict with every other piece of evidence we can find, we have to conclude that it is most likely false. Perhaps he wasn’t aware of conditions on the ground, but if that were the case, we’d expect him to say as much, not to confidently assert things that aren’t true.
And just as we thought we had heard it all, the NEJM paper on the TOGETHER Ivermectin trial got a small update, adding a “limitations” section. This contains such relevant gems as:
…off-label use of ivermectin is promoted by paramedical groups…"
What's a paramedical group? Are there groups of paramedics, going around in ambulances, throwing pills at people? The implication that there aren't actual doctors promoting ivermectin is disgusting. But it gets much worse.
…and is widespread in Brazil.
Wait. What "paramedical group" was promoting this off-label use in Brazil, where the trial took place? Could it be... The Brazilian Ministry of Health? Maybe the Brazilian Federal Board of Medicine?
Here’s what a paper in The Lancet has to say about that:

I’m not sure how such claims are even allowed to be published. But let’s move on to our second question.
How Were Patients Excluded?
The normal way patients are excluded is by having an inclusion/exclusion criterion citing the reason for the exclusion. And yet, the original registration for the TOGETHER trial did not mention any exclusion of patients for recent use of ivermectin, nor did any of the many subsequent revisions of the protocol revise it to state an exclusion of such patients.
The presentation of preliminary results on August 6, 2021 also did not mention exclusion for ivermectin use.
In the paper’s discussion section, the authors—for the first time—indicate there was some kind of filter:
We ensured that trial participants did not have a history of ivermectin use for the treatment of Covid-19 by means of extensive screening of potential participants about this issue.
This is quite the curious sentence. First, an exclusion for ivermectin use is not present in any of the protocols, in the pre-registrations, or in any discussions prior to this paper. Secondly, the qualifier “for the treatment of Covid-19,” implies that use of ivermectin for other reasons was not cause for exclusion.
Given that the Case Report Form filled in for each patient did not have a dedicated question on ivermectin use, we can only assume that they got their information from the concomitant medications section. In this section, there is a field to fill in for the “indication,” for which the medication was used. So if a questionnaire included ivermectin as a concomitant medication, with Covid-19 as the indication, perhaps the patient was excluded, either at the time or after the fact. However, given that this trial has had trouble collecting data on things as basic as age and time since symptom onset, it’s hard to believe that indeed the concomitant medications and the specific indication was filled in correctly for all patients, especially when this was not called out as an explicit exclusion criterion.
Given that this was never written in the trial protocol, even if it was done, it’s arguably a protocol violation. At the same time, in the limitations section that was later added to the NEJM article summary, the authors wrote:
The authors attempted to screen potential participants for previous ivermectin use.
Obviously, “attempted” and “ensured” are very different words, with wildly different implications for the trust we can place on this trial. Someone must provide details about exactly what was done.
Has the principal investigator said anything?

First of all, note that he’s speaking to a slide that names “Use of study drugs for COVID” as an exclusion criterion. This is the first time such an exclusion criterion is named anywhere. It’s not in the protocols, or the ethics approvals, or the registrations, or the papers themselves. It’s not in any public record of the trial. And there’s a lot of them. What’s more, the way it’s written implies it applied to all the other arms. Did they, too, have unwritten exclusion criteria?
Here are the precise words he used:
We had a number of exclusion criteria, but one of the exclusion criteria that I think will meet some of the questions people have got is “have they been exposed previously to ivermectin?”. In our trial we had questioned quite closely about people’s exposure previously, and we excluded anybody that had previously taken ivermectin for their COVID, or were likely to take it
The plot thickens. Apparently, not only did they exclude people that had taken ivermectin for COVID, they also excluded people who were likely to take it.
I have absolutely no idea how that could be done—even in principle. Anything that comes to mind is so rife with potential for abuse that my mind halts and refuses to consider it.
So which is it? Did they exclude for use of suspected future use, as Mills said? Did they “ensure,” as they say in the discussion section of the paper? Did they do nothing, as in the exclusion criteria (the obvious place for such information)? Or did they "attempt to screen," as is written in the limitations section of the new summary?
Whatever it was, as in Lopez-Medina, we also observe a characteristic pattern in the adverse events section: Gastrointestinal disorders, a typical side-effect of taking ivermectin, were substantially higher in the placebo group, raising more questions as to whether the placebo group was getting the benefit of ivermectin use outside the context of the trial.
Could Things Be Even Worse?
Stepping back for a second, a certain reticence to exclude ivermectin users makes a lot of tactical sense for all the reasons mentioned in the Nature article: eliminating patients who used ivermectin would drastically dwindle the patient pool, and the TOGETHER trial was testing drugs other than ivermectin at the same time (fluvoxamine, metformin) that would also have to be impacted. Patient throughput is essential for a large-scale adaptive platform trial.
If they did try to avoid enrolling people with admitted use of ivermectin for COVID to the ivermectin arm, could they have done it in a way that didn’t affect overall enrollment? The reply by Dr. Ed Mills to Steve Kirsch, which we mentioned above, contains a hint that they may have done just that:
All patients were asked about their previous ivermectin use and excluded if they reported ever using it for COVID. Patients did not choose which intervention they received, but could be blocked from receiving one if they previously had taken it. This is all in the protocol.
This answer raises far more concerning questions: were patients who had taken ivermectin “blocked from receiving it?” Looking at the protocol for any hints of such an operation, I found this: in one version of the protocol, there is a bit about reassigning patients between arms. Here it is:

Here are the specific words used:
The randomization system will be programmed to block the randomization of diabetic patients in the metformin arm if:
Patients taking metformin at dose > 1.5 g/day
Patients with clinically important renal insufficiency or documented creatine > 1.8 mg%
I notice that both Mills and the protocol use the verb “block” for the operation of disqualifying a patient from eligibility in one arm, while not completely excluding them from the trial as a whole, so I will assume they are talking about the same thing.
If indeed patients taking ivermectin were “blocked” from being randomized to the ivermectin arm, then we have two possible cases for their reallocation:
They were re-allocated to another treatment arm, which for most of the duration of the high-dose arm would mean that they were re-allocated to the fluvoxamine arm. This would be incredibly bad research practice, given that the investigators must be assumed to have held a belief that ivermectin was likely to help treat COVID (if they didn’t, why were they dosing patients with it?). The question then becomes how many of the fluvoxamine patients were taking ivermectin also, and, to my knowledge, we don’t have any such data.
They were re-allocated to the placebo arm, which would, as a result, water down any effect the ivermectin treatment might have.
I have a hard time deciding which of these cases is worse. Ultimately, I’m baffled. the investigators may have been between a rock and a hard place here, but that doesn’t excuse them compromising the results of all their studies in order to avoid aborting the trial or relocating it when they realized this would be a problem.
Consider this: even if the investigators managed to completely exclude anyone who had recently used ivermectin, for instance by performing appropriate blood tests, that *still* doesn’t make the issue go away: the very exclusion would create a selection bias. Considering that people who take ivermectin may be more likely to cluster into different socioeconomic, political, or even biological categories, regardless of the reason, would affect the results of the trial, even if none of them were included in the trial.
Conclusion
We need someone to somehow clarify what in the world was done to patients who indicated they had taken ivermectin for COVID. The messages coming from the investigators are so contradictory as to cause one’s hairs to stand on end. Were patients taking ivermectin excluded? Were they reassigned to placebo? Were they reassigned to fluvoxamine? If nobody will answer these questions, we need to see the data so we can make some sort of determination.
But, of course, the data is still absent, over a year after the original release of the results of the ivermectin and fluvoxamine arms.
The fact that people are not raising hell about this may be the most concerning fact of all.
Summary
Pulling it all together, we have:
A near-certainty that ivermectin was used in high amounts in the area at the time of the TOGETHER ivermectin trial.
Contradictory statements on community use by the principal investigator and the text of the publication itself.
Absence of ivermectin in the exclusion criteria of the trial in all versions of both protocol and registration.
Contradictory accounts of how the organizers of the trial handled patients who had been taking ivermectin, all of which are highly problematic for different reasons.
An indication that patients who had taken (or were likely to take?!) ivermectin for COVID were re-allocated to fluvoxamine or placebo, compromising the entire trial.
I’m out of words, draw your own conclusions.
•••
(End of quoted article by Alexandros Marinos.)
In Part 2, G-d willing, we will bring in-depth coverage of the amazing story of how Uttar Pradesh, India’s largest state, with a population of 231 million, (over 2/3 of that of the United States), virtually eliminated covid through systematic government-sponsored use of ivermectin, but this historic accomplishment was not covered by mainstream media.
Link to Alexandros Marinos’ original article:
I've never been able to grasp why people give governments the power to prevent them from taking any medicine or treatment that they wish at their own risk. People have always engaged in risky behaviors, whether for the purpose of improving their health or just for fun and pleasure. How is it the business of any agency to tell people what they cannot do when it effects only themselves?
The past few years have basically destroyed my faith in humanity's common sense and survival instinct.