


This creeps me out: The evil trap of mass BRCA testing
Something is wrong over here.

BS”D
I’m not a Rabbi, scientist, or doctor, but I don’t think anyone has to be one of those to see the grave net harm that mass BRCA screening will cause to society.
Note, I’m not going into early cancer detection screening here (although I have to admit suspicions that all isn’t above board in that field.) I’m also not even dealing with the question of an individual who wants to test themselves genetically because multiple family members have died of cancer.
Rather, this is about the same public health authorities whom we’ve learned not to trust, now promoting mass genetic screening of the population of healthy individuals - in this case, of the Ashkenazi Jewish population - to find the “one in forty” they claim carries the BRCA mutation. And they want to start testing people really young - like, 18.
In the UK, the NHS is targeting Ashkenazi Jews first for genetic testing. https://www.bartshealth.nhs.uk/news/making-an-impact-in-breast-and-ovarian-cancers-5384
Sadly, the Jewish news sites are proud and excited about what the NHS is doing for them.
Personally, I quite suspect sinister motives on the part of the NHS, I’m sorry to say. If you’ve been reading the articles in this column, you know that the NHS is keen on decreasing the population, not on saving lives.
In the US, the CDC is also overly concerned about Ashkenazi Jewish cancer risk, and encourages genetic testing. This is the same CDC who kept most of the country from using safe, decades old repurposed drugs to treat covid, killing untold numbers of people, and then murdered even more with the “vaccines.”Are we now to believe that they’re suddenly pious lifesavers? Something doesn’t smell kosher. https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/hereditary_breast_cancer/jewish_women_brca.htm
What will be the results of mass genetic screening of the Ashkenazi population? Since they claim that one in forty carries the defective gene, that’s 2.5% of the population. So, out of every 100,000 people tested, 2,500 will be told that they carry the mutation, and are likely to die of cancer. Out of 1,000,000 people tested, 25,000 will receive the “joyous”news.
Then what?
They will have to carry that knowledge around forever. It will impact them and their families in innumerable ways.
“Genetic counseling” will be offered to discuss the “options.” Of course, highly recommended will be early, “lifesaving” removal of breasts, uterus, and ovaries.
Established management strategies for high-risk individuals include: 1) risk-reducing salpingo-oophorectomy (RRSO) to prevent tubal/ovarian cancer (hazard ratio [HR] = 0.21) (which also halves breast cancer risk in premenopausal women) (6), 2) risk-reducing mastectomy to prevent breast cancer (7–9), 3) early onset breast screening (MRI/mammograms), and 4) preimplantation genetic diagnosis.
https://academic.oup.com/jnci/article/107/1/dju379/907914 (Notice that “preimplantation diagnosis” is also offered. This means that parents doing IVF can screen their embryos for BRCA mutation (and presumably discard the babies who have the mutant gene.)
Will all this have a net positive impact, in which more people are alive, healthy, happy, building families and thriving?
Or will it have a net negative impact in which more people live in fear, dread, depression, and isolation, fewer children are born, and in the end, there are less people?
I have no doubt that it’s the latter. And I also believe that’s the desire of those pushing the program (along with all the money to be made from the surgeries and the Pharma-dependent people they create with every BRCA-mutant diagnosis.)
Let us examine the predictable devastating societal effects. We don’t need a fancy study to tell us these things. We can simply use our brains. Any “study” that shows the opposite has to be flawed, because the following is simply logic.
Since I’m part of the Torah-observant community, I speak of what I know in my community, where marriage and having a large family are the normal trajectory of life.
1) The women who are yet unmarried when they get their life-altering news may experience difficulty finding a suitable husband, because they now have a “health problem” they need to disclose, which may cause their early death.
2) Single or married, anyone who is informed of their BRCA status is likely to go through a prolonged period of upheaval, depression, and difficulty functioning, as they struggle to make the life-altering decisions they’re pushed into.
2) Some women will opt to listen to the doctors “best recommendations” and undergo double mastectomy, hysterectomy and oophorectomy (removal of uterus and ovaries.) Obviously, they will be physically unable to have children anymore.
3) Some of these women’s marriages and lives will spiral downwards after their “lifesaving” surgeries.
4) Some women, while told they don’t have to remove everything just yet, will be afraid to bring children into the world since they may be orphaned young.
5) Some women will be told to go on Tamoxifen long term as a preventative for breast cancer. They’ll be told to use contraception, as while on this medication one may not become pregnant, since Tamoxifen is dangerous to the developing fetus.
6) Most of the women will go around for the rest of their lives in fear of death and/or feeling they have a stigma. Aside from the ruined lives, will that fear of cancer and the hyper-focus on it, perhaps create a self-fulfilling prophecy?
I am unclear as to what surgical interventions they will offer men who test positive for the BRCA mutation and supposedly have a higher risk of pancreatic and prostate cancer, and melanoma. (I don’t think it’s recommended as of yet to remove the pancreas, or skin, prophylactically. 🤔 Maybe soon, though?)
Some thoughts: I feel that this whole approach comes from an ignorant, misguided, G-dless, fatalistic attitude which accounts for neither nutrition nor prayer. It’s all about the genes, and if you’re “stuck” with “defective genes” it’s pretty hopeless… unless you go under the “expert’s” knife, of course. What about the humility of acknowledging the Creator as the only One determining the length of our days… recognizing that we need to leave some things to Him only - that maybe poking around in the genome for these purposes is overstepping our boundaries.. that living life the way He wants us to - happy, intact, building a family - is the right option, rather then endless testing which will lead to a very different life… What about prayer, positivity, and increasing our merits? Faith that G-d decides our lifespan, not our genes. Sure, we’re obligated to do our part, but is checking our genes and cutting off our body parts really considered “doing our part” in G-d’s book?
Will this testing and prophylactic removal of organs even “save their lives?” Not necessarily! People could still develop cancer anywhere else in their bodies, that hasn’t been cut out yet. Or, they could die of a heart attack or stroke, with perhaps greater risk of doing so, from the stress and/or the hormone replacement therapy they may need to be on.
😰😰😰😰😰
(Maybe the “safest” of all is to just apply for MAiD? They promise it doesn’t hurt.)

Rather than this destructive spiral, wouldn’t it be better to counsel the whole population in healthy eating, and in natural supplements that are anti-cancer, (such as helping with mitochondrial damage, likely the root cause of cancer), as preventatives, instead?
Disturbing thought: Who knows if the results they give will even be true?
(Thinking of the PCR tests…)
And, who is to say that their “research” showing that their interventions “save lives,” is honest?
Some excerpts from this BMJ article:
Time to assume that health research is fraudulent until proven otherwise?
July 5, 2021
Health research is based on trust. Health professionals and journal editors reading the results of a clinical trial assume that the trial happened and that the results were honestly reported. But about 20% of the time, said Ben Mol, professor of obstetrics and gynaecology at Monash Health, they would be wrong. As I’ve been concerned about research fraud for 40 years, I wasn’t that surprised as many would be by this figure, but it led me to think that the time may have come to stop assuming that research actually happened and is honestly reported, and assume that the research is fraudulent until there is some evidence to support it having happened and been honestly reported. The Cochrane Collaboration, which purveys “trusted information,” has now taken a step in that direction.
As he described in a webinar last week, Ian Roberts, professor of epidemiology at the London School of Hygiene & Tropical Medicine, began to have doubts about the honest reporting of trials after a colleague asked if he knew that his systematic review showing the mannitol halved death from head injury was based on trials that had never happened. He didn’t, but he set about investigating the trials and confirmed that they hadn’t ever happened. They all had a lead author who purported to come from an institution that didn’t exist and who killed himself a few years later. The trials were all published in prestigious neurosurgery journals and had multiple co-authors. None of the co-authors had contributed patients to the trials, and some didn’t know that they were co-authors until after the trials were published. When Roberts contacted one of the journals the editor responded that “I wouldn’t trust the data.” Why, Roberts wondered, did he publish the trial? None of the trials have been retracted.
Later Roberts, who headed one of the Cochrane groups, did a systematic review of colloids versus crystalloids only to discover again that many of the trials that were included in the review could not be trusted. He is now sceptical about all systematic reviews, particularly those that are mostly reviews of multiple small trials. He compared the original idea of systematic reviews as searching for diamonds, knowledge that was available if brought together in systematic reviews; now he thinks of systematic reviewing as searching through rubbish. He proposed that small, single centre trials should be discarded, not combined in systematic reviews.
Mol, like Roberts, has conducted systematic reviews only to realise that most of the trials included either were zombie trials that were fatally flawed or were untrustworthy. What, he asked, is the scale of the problem? Although retractions are increasing, only about 0.04% of biomedical studies have been retracted, suggesting the problem is small. But the anaesthetist John Carlisle analysed 526 trials submitted to Anaesthesia and found that 73 (14%) had false data, and 43 (8%) he categorised as zombie. When he was able to examine individual patient data in 153 studies, 67 (44%) had untrustworthy data and 40 (26%) were zombie trials.
Others have found similar results, and Mol’s best guess is that about 20% of trials are false. Very few of these papers are retracted.
We have long known that peer review is ineffective at detecting fraud, especially if the reviewers start, as most have until now, by assuming that the research is honestly reported. I remember being part of a panel in the 1990s investigating one of Britain’s most outrageous cases of fraud, when the statistical reviewer of the study told us that he had found multiple problems with the study and only hoped that it was better done than it was reported. We asked if had ever considered that the study might be fraudulent, and he told us that he hadn’t.
We have now reached a point where those doing systematic reviews must start by assuming that a study is fraudulent until they can have some evidence to the contrary.
Richard Smith was the editor of The BMJ until 2004.
Some personal stories from some people on my chats will illustrate how real the effects of BRCA screening are:
S. related: “A friend from childhood’s mother died from “cancer” (aka vax injury) last year after being completely healthy for 81 years. (Never went to doctors, was a “health nut” who was happy and ate well). While undergoing cancer treatment for 14 months, they scared her and she told her daughter, my childhood friend, that she, too, needed to get screened for cancer. So my friend, also never sick (except for covid vax injury) now went to be screened, and what do you know? She is “BRCA breast cancer” gene carrier, out of the blue, and is scheduled to have both her breasts removed “just in case.” It’s CRIMINAL! They are obsessed with experimenting on and mutilating child-rearing bodies!”
M. said: “My father died of pancreatic cancer. Thank G-d, I tested negative for BRCA, but one of my sisters was positive. They had her get a hysterectomy and ovaries removed and said that that would lower her chance of breast cancer tremendously... She is post having kids, but they recommend by 35 to have everything removed.”
Unfortunately, the mass genetic screening has begun in the Jewish community. I was sent this picture of an event which happened in the Crown Heights section of Brooklyn, NY, on December 28.
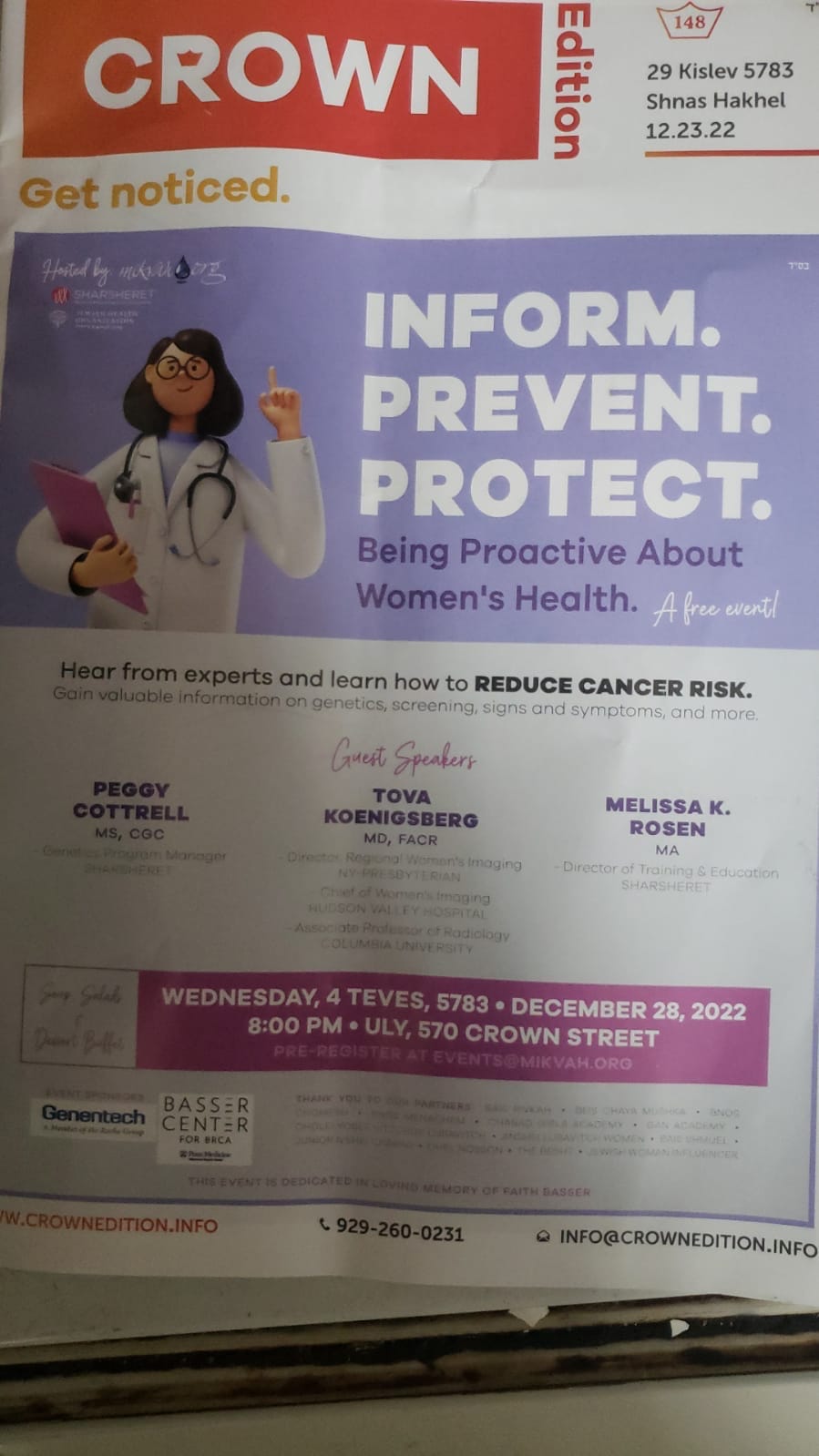
This event was run by a trusted organization within the Jewish community. They surely think they’re doing something positive.
The question is this: These screening events cost a tremendous amount of money to advertise and to run. Where does the money originate from? Is this somehow coming from the CDC? We did not find evidence of that so far, but I am very suspicious. Is there another, private, entity with malevolent intentions funding this?
The problem is that when community-based organizations run these programs, people trust. Nobody is thinking that this is likely to be the result of an agenda originating outside the community, an agenda they may not appreciate.
In the case of the Crown Heights screening ad above, we notice several organizations who partnered with the small community organization that hosted. The community organization is used to gain access to the population.
I’ll include each partner organization with whatever preliminary information we have for them.
I reach out to you to help us research and figure out what’s going on, if you have the know-how.
Genentech - the Biotech company listed on the ad
Does the idea of handing over the genetic database of a population that has been historically targeted for destruction make you concerned?
It seems like a very foolish move to me.
Genentech is a huge operation, a subsidiary of Roche. While Roche is supposedly American, it’s headquarters are in Basel, Switzerland. Hmm.
I am getting a feeling of deja vu, as Roche is reminding me too much of the German IG Farben pharmaceutical+ cartel between the World Wars, in which the true nationality of many of the companies was purposely hidden. That IG Farben cartel was so powerful that they are the ones who brought Hitler to power with their enormous money and undercover influence - and they continued running the show behind the scenes. IG Farben also ran Auschwitz and other extermination camps. The empire regrouped after WW2 despite being broken apart and sold off because of pervasive Nazi ties. It’s a very eye opening story and worthwhile to know, and is detailed in the book “World Without Cancer.”
That’s just another reason that this whole thing just seems all wrong.
https://www.gene.com/
https://en.wikipedia.org/wiki/Genentech
Here was some preliminary financial research that someone started for me on Genentech.
https://www.guidestar.org/profile/46-0500264
https://www.usaspending.gov/search
https://www.usaspending.gov/award/CONT_AWD_75A50322F80028_7505_V797D60724_3600
Basser Center
https://www.basser.org/related-organizations
Basser Center is part of Penn Medicine, which is part of University of Pennsylvania Health System.
The University of Pennsylvania Health System (UPHS) is a major multi-hospital health system headquartered in Philadelphia, Pennsylvania. UPHS and the Perelman School of Medicine at the University of Pennsylvania together comprise Penn Medicine, a clinical and research entity of the University of Pennsylvania.
https://en.wikipedia.org/wiki/University_of_Pennsylvania_Health_System
https://www.pennmedicine.org/
The Basser Center for BRCA was established at Penn Medicine’s Abramson Cancer Center in 2012 by Penn alumni Mindy and Jon Gray, whose total giving to the center is $110 million. Their visionary gift grows stronger every day through the commitment of our generous donors and philanthropic partners.
OneInForty is partners with Basser.
Oneinforty is a nonprofit organization dedicated to stopping BRCA-related cancer in its tracks. To advance this mission, Oneinforty raises awareness among Ashkenazi Jews of their high risk of inheriting cancer-causing BRCA gene mutations and provides the support individuals and families need to face this risk, prevent cancer and detect cancer early.
https://oneinforty.org/
http://www.myjewishgenetichealth.com/
Sharsheret
https://sharsheret.org/ is promoting breast cancer awareness in the Jewish community.
What we have noticed is that those who are pushing the extreme medical interventions such as BRCA screening and preventative organ removal, even if they are Jewish and call themselves “Torah observant,” invariably have integrated so deeply within the medical/woke establishment that their values don’t seem to be aligned with traditional Torah values.
According to Usa Spending, Sharsheret received a grant (spanning 2019-2024) for 1.5 million dollars for “Link Program - Outreach and Education Initiative: Multiple Approaches to Support Young Jewish Breast Cancer Survivors and Jewish Metastatic Breast Cancer Patients.” https://www.usaspending.gov/search/?hash=5dae027f8bfed3aa888ea8fbae47fc1e
Sharsheret also received 3 other grants from the CDC in recent years. https://www.guidestar.org/profile/13-4198529 https://njconsumeraffairs.state.nj.us/public-charity-search-results/
I will assume that Sharsheret is trying to do good work and save lives, to the best of their (unbeknownst to them) limited knowledge.
Regarding the CDC, there’s no room to give the benefit of the doubt, as they’ve repeatedly shown themselves to be murderous.
What is the ultimate goal of the CDC and NHS? What do you think?
Please share your research, thoughts, and stories in the comments.
Please note that this article discusses my views about community-wide genetic BRCA testing. I am not a doctor and make no recommendations regarding individual patient screening decisions.
Thank G-d, my Rabbi’s eyes are very wide open. He reviewed my article and feels VERY strongly about the topic. I’m positive that many Rabbis will see the evil of the BRCA testing program as well as soon as it’s presented to them.
Thank you for this. It reaffirms my decision to decline mammography and genetic testing of any kind. I have come to believe that the current state of medicine is a religion based on the worship of science and the fear of death.