


WHAT’S REALLY HAPPENING NOW IN HOSPITALS? 😱
And exploding casket orders, and much, much more

BS”D
The seal of G-d is TRUTH. By working to spread the truth and save lives, you are a messenger of the Creator of the World. Remember that and take strength from it.
Dr. Pierre Kory wrote another segment on Friday in his reports from nurses telling the truth about the explosion of cardiac arrests, cancers, strange illnesses, and more. This is a must-read:
Reports From the Front Lines of the Vaccine Catastrophe - Part 2
Increasingly shocking evidence of the impacts of what Ed Dowd suggests we should start calling a "mass democide" (death by government) continues to emerge.
Jul 8

In Part I of my “Reports from the Front Lines of the Vaccine Catastrophe,” I relayed first hand information from senior nurses who work in emergency rooms, hospital wards and intensive care units regarding unprecedented amounts of young people presenting with cancers, strokes, and heart attacks. For a brilliant, succinct layperson’s explanation as to the pathophysiology of how and why these medical events are occurring, please read this substack post by my friend and colleague Dr. Kevin Stillwagon (he is also an airline pilot).
My main source for the more detailed reports is a senior ER/ICU nurse who has been carefully observing and documenting the presentations and problems occurring in the care of vaccinated patients presenting to a major academic medical center. She has continued to discreetly and prudently extract information from a huge network of colleagues she has built over her career. She responded to my last post, adding new, even more alarming information. Here goes:
(*I have spelled out all abbreviations and inserted explanation of some terms)
6/15/22: Thanks for getting my input out there. More cognitive dissonance showing, though. I'll have more very soon - picked up a bunch of weekend night shifts on cardiac units - 2 separate ones. I just found out they added multiple crash carts to every unit in entire hospital. That costs a bundle. And is another red flag.
One more thing....that VAXXED label is showing up for research participants, as I wondered if that were the case. Can't say that is the only use of the very prominent positioning of it on patient chart, as those were indeed "challenging cases" not otherwise explained. And nursing notes are still being used to note patient’s request to enter their vax lot numbers and which vax they received, and where if they obtained outside of our system - boosters as well. Pt just wants it noted in the chart - little do they know it doesn't count.The commenter who said there are no billing codes for "vax injury" discussions is absolutely correct. The elephant in the room is simply not billable!
6/24/22: So crash carts first: One way to find out (whether they had indeed added more cardiac arrest carts) proved to be walking specific units. Yes, many were added, especially those whose unit design is one long, long hallway with no way to see who is close by when you hit the code (cardiac arrest alert) button or yell out for help - they had to populate with more carts. Poor planning and design when built just a few years ago. (But that doesn't surprise, Pierre. For our massive cancer hospital, they never put oxygen access in the walls, NOR was the wall suction installed for nasogastric tubes, etc. The valves in rooms were never hooked to anything until ...oops, last minute shut down of sections of each floor to fix that massive mistake .Delayed opening of cancer hospital and neuro floors - Disaster.). So for the carts, they have added more mostly on poorly designed units, but those within the existing hospital structures they couldn't change . We have off-shoot ICU sections that were late converts to ICU capability and they had to have cart augmentation for sure. Carts are often parked outside the rooms of those we expect a crash (cardiac arrest) at any time, or have arrested earlier in the shift. Change out and restocked and sits there just in case. So that cart is effectively dedicated to that patient for the shift at least.
The supply coordinators:
Second was going to the supply coordinators who have to physically come up and change out each crash cart. Each time. Each unit, sometimes multiple times a night. For YEARS at night, there was only ONE person per whole section of hospital, often running them thru our underground tunnels to far flung sections. We have ATS (automated transport system) but crash carts are forbidden to be sent this way. They must be physically delivered and taken back the same way to be cleaned and restocked using a check off list, patient labels for charge items, etc. You know the process.
Since this increase in codes, even if cart was not cut open, they've had to hire dedicated supply coordinators at NIGHT and more pharmacy staff dedicated only to restock and verification/cross check status each cart - the integrity of each. Some drugs are no longer sent by pneumatic tubes and are being sent on cart, if not already in Pyxis (unit located pharmacy dispensing system for nurses). Someone must physically be with cart at all times in that case. I saw security with pharma staff and cart, just this weekend. Our old SICU area has its own separate way of handling carts and codes internally, so I do not count them. Transplant floor lung/heart - ECMO, etc - already had multiples.
We have implemented universal beds (a standard hospital room that can be converted to ICU capability to take care of sicker patients) in almost every new part or renovated part since 2009. Flip the wall behind the patient and it's fully converted.. But waiting for a new cart to come up when you only had two per unit and now multiple events - that was a liability they did not want to absorb. It's not the expected-to-arrest and still full-code status patients that are circling (the drain), it's the never expected to code patients - younger ones especially - that drove this decision.
Med Surg floors also got more carts, b/c they are getting more complex patients sent to them. I call it level-of-care-creep.. Greater complexity, but never have they altered the RN:Patient ratios to accommodate the higher level of care. Many RNs there are new, untrained to carry out orders now being placed for these patients whose illness or disease process they never would usually see on a Med Surg floor. They are pushing limits on allowable infusions, titration to higher doses, etc and it was a point of discussion that some nurses just are not comfortable. But, you fired a chunk of your staff who refused vax - they were the more experienced providers of all levels and you now have newbies who can't manage the care levels especially when their patient ratios are not altered, no training. It's a problem. Add in a few codes.... a mess. We have a very strong nurses union and this will be changed. Asking newbie nurses to work out of their scope of training or needed certification puts patients in danger, especially when they have "weird issues" - Charge Nurse I've known for years on one of these units said they just have not seen the clotting issues they have now before, with difficulty doing peripheral blood draws on patients who she thought were just Covid recovered. Turns out, looking at charts, they are reporting vax/boosters but IT'S IN THE NURSING NOTES WHERE PTS ARE REPORTING IT, and must be documented as a patient communication to Nursing. If they got vax/boost at our facilities, it's already clear in the chart that it is so. She ( a senior head nurse did not even notice this fine little detail. It's buried several layers down in the EMR (the hospitals electronic medical record system). So I believe many (nurses and doctors) are seeing them as unvaxxed, instead they are led to think it is just Covid-related issues post-recovery, as they are not seeing the patients real vax status. Supports that narrative of unvaxxed being cause of oh, EVERYTHING IN THE WORLD.
This last issue above (deeply explored in Part I) describes the inability of nurses to accurately document a patient as being vaccinated upon admission to the hospital.
This fraud has been crying out for an investigative reporter (out of the 10 left in the world) to look into who and how the Federal Health Agencies influenced the process for documenting vaccination status newly admitted hospital patients across the country. Electronic health record systems in major hospitals across the country followed the same (ridiculous) process: if you were vaccinated in a physicians office that was employed by that hospital, and the physician was connected to the same electronic health record, and the physician or nurse documented it in the electronic health record, you got recorded as “vaccinated”. However, if you had your vaccination anywhere else (most people), even if you had your vaccination card on you or could remember the date and location where you got the jab, you got documented as “unknown” on the main screen of the health record.
In those cases, the patient’s vaccination status gets placed in the “nursing notes” section where no-one looks for it. All of these patients documented as “unknown” were interpreted by all the health care providers as “unvaccinated.” In this way, the majority of doctors and nurses were led to believe that everyone in the hospital was unvaccinated. It also allowed our federal health agencies to create and disseminate charts and graphs showing the hospitals purportedly filling with unvaccinated people (I actually believe that even these data were further manipulated). The impact of this widespread fraud fueled the vast majority of doctors to hector anyone and everything to get vaccinated. Unclear how much blame to assign them on this as it took me a while to figure out why no patient in my ICU ever had a “vaccinated” status on the front screen of their record. Anyway, moving on:
The unit I worked on had float staff I never met, but mostly long-term coworkers and we are all of the same mindset. I kept quiet around the float pool folks until later in night when they had their own stories to share about pts. All of them confirmed what we've all seen - none of it makes sense unless you go to the 800 lb elephant in the room. The vax cheerleaders on staff - never hear a peep from their end. I know some have buyer's remorse for pushing family to get vaxxed, and no need to dig into that wound. Long Covid is only term allowed, no vax injury.
This last comment really got me. The standard practice is to describe all the strange illnesses as “Long haul COVID” rather than mRNA “vaccination injury syndrome.” Of course that is what happens. Entirely predictable and so so sad.
There is a Long Covid study many employees as well as patients are participating in - I know two employees in it. Don't know that it is providing them any answers to their disabling issues, especially at their young age, but they're hopeful. They are true believers - got fully vaxxed and boosted and will continue to do so. And they continue to contract Covid variants. Pass it along to the rest of the same vaxxed-up cohort. Rinse and repeat. To bring up data that points to the exponential and cumulative harm is just pointless. They want to die on the hill of believing they did the right thing, no matter what their bodies are telling them. Until they can no longer do so.
ED doc - got him pulled aside but we had to go outside to talk. And yes, phone off. In ED, pt issues are discussed in a kind of code where it concerns vax injury as probable cause. Administrators wander through at all hourr so open discussions are just not happening. Residents are getting more frustrated - I guess its showing in staff meetings b/c they are seeing data and pts are bringing in data. Shift hand-off report can get tense, I was told. (Many suffering from the cognitive dissonance "I have hundreds of thousands in med school loans out. I cannot deviate or I lose everything and still owe all that loan money back. Must stick to what I am told") They become check-box doctors at that point. You either sell your soul, or seek your own data and research and then join the "French Medical Resistance" - not an easy call for a 20-something to make. Not every patient is willing to walk in the dark about the very severe issues they are having, with PCPs telling them it's nothing to worry about. The push back is real from patients that chose to be informed and the ED docs have to find a way to address this at their level before they admit a pt or discharge with some vague diagnosis. I see future liability coming as the data keeps pushing out. More patients are asking for their FULL medical record. They know. They know. All the other stuff is still happening. Still have no space in cancer hospital side for the explosion of pts needing treatment - it is NOT b/c they delayed treatment due to the pandemic. It's because they just received a diagnosis that requires immediate intervention. Not from delayed screening or treatment initiation. According to the same case manager I spoke with weeks ago that is carrying a pt load of almost 1000 pts now, she is trying to get creative and find space at outpatient facilities closed on weekends and schedule her teams and patients to go to those sites with full equipment when it's appropriate to get infusion at least. This is crazy. She called asking if we could open up space in a specific area - and yes, we are doing it.
Here, Dr. Kory reposted parts of Etana Hecht from Clown World’s latest article. I was also going to share it, myself, so I’ll include more pieces, too.
"A Peasants Revolt"
FDA and the CDC are on Notice/The Casket Industry is Booming
Etana Hecht July 6
Caskets
I spoke to the family who owns one of the largest casket manufacturers in North America. They supply caskets to huge chains across the US and manufacture Prime Caskets, among others. It’s horrific to have to report on such a thing, but the owners said that their sales of typical caskets have increased by 20%, and since Dec 2021 their sales of small-size caskets (under 5 feet, i.e, for children) have increased by 400%. He’s not the only one talking about it, those in the funeral industry are well aware of the sudden change in the nature of their business.


For the first time in over 30 years in business, they’ve begun to receive orders for small-size caskets in bulk. That sentence makes me nauseous to type, so armed with that painful piece of information, let’s focus on the tremendous efforts to keep the kids healthy. Of course, the casket numbers themselves aren’t proof that the vaccine is harmful or fatal for some children, but it sure is yet another blaring red signal.
Switching back to Dr. Pierre Kory for a bit:
Blaring red signal… among many blaring red signals. Pilot death data is blaring too.
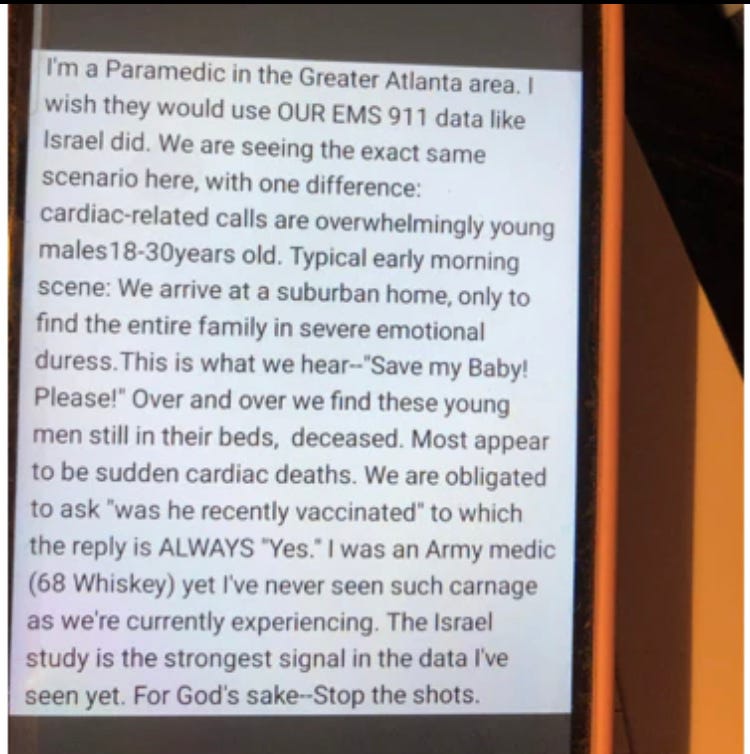
Apparently, there is a reporter from Canada who is actively seeking reports from emergency medical technicians, funeral home directors, embalmers, and nurses on Twitter and other social media. He appears outraged that the “main stream media” has been ignoring these data. What is this, the first mainstream journalist to wake up and have courage to address the global democide? Here is one of the direct messages to him from a very concerned paramedic:
The above is supported by new, massive demands for ambulances across the world, evidenced by this compilation of TV news and print reports of shortages, compiled in another favorite substack of mine by Marc Crispin Miller. Note that although some reports blame the issue on shortages of staff and ambulance parts, the vast majority also mention… increases in the number of calls for ambulances. Hmm.

Back to a text exchange with my “source” during one of her shifts referring to the ambulance/emergency services issue:

Now let’s switch to more positive stuff (sort of?). This bombshell news article from a major newspaper was posted by Robert Malone. I find this headline unprecedented and evidences a clear “crack" in the dam of propaganda and censorship… A trickle.. will hopefully become a river:

That trickle may be starting to flow.. now two more major UK newspapers addressing all the “unexplained” dying:

https://www.independent.co.uk/news/uk/holyrood-covid-b2032847.html

https://www.telegraph.co.uk/news/2022/07/05/excess-deaths-rise-not-covid/
Switching back to Etana Hecht’s article:
On Offense
Dr. Naomi Wolf appeared on Warroom and announced some positive developments in the efforts to save children from the Covid vaccines, amidst a flurry of activity as the responses to the FDA authorization of Covid vaccines for babies ramp up. As Steve Bannon put it, this should be a “peasant’s revolt against the administrative state”, and thanks to the efforts of Daily Clout and its supporters, along with other amazing grassroots organizations, that’s exactly what’s happening.
https://rumble.com/v1b7grf-dr.-naomi-wolf-we-must-revoke-covid-19-injections-for-children.html
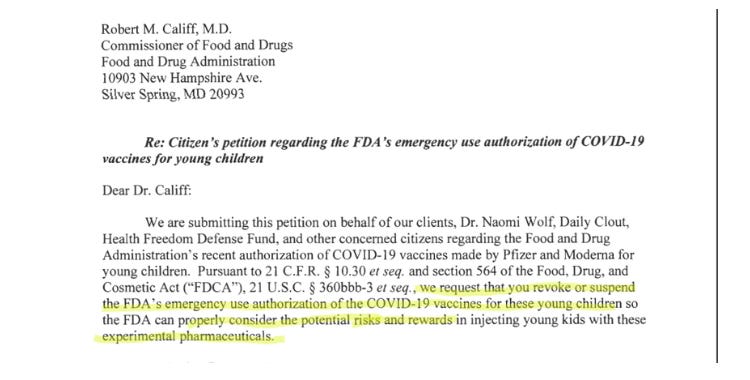
“A Shot Across the Bow”: Dr. Naomi Wolf of Daily Clout and the Health Freedom Defense Fund fund filed a citizen’s petition with the FDA to request a reversal or suspension of their EUA for Covid-19 vaccines for children. They requested attention for the more than 130,000 comments regarding the EUA that were submitted by the public. Scott Street and John Howard are among the attorneys who successfully put a stop to the forced masking on airplanes, to the huge relief and gratitude of millions of people. They’re now representing Daily Clout and the HFDF in the efforts to end the Covid vaccines for children.
The letter included a part from Dr. Naomi Wolf herself, where she notes the negligible risk of Covid-19 for children and the fact that neither safety nor efficacy has been proven for the vaccines. Healthy kids are more at risk from seasonal flu than Covid, and there’s no justification to expose the kids to the known and unknown risks of an experimental vaccine. The letter ended with a fantastic line from the lawyers:
“The FDA is charged with protecting public health, not marketing the products of arguably the most powerful industry in the world.”
The petition can be read here:
https://healthfreedomdefense.org/dailyclout-and-hfdf-file-citizen-petition-with-fda/
Additionally, The Children’s Health Defense has also served a legal letter to the FDA to halt the children’s Covid-19 vaccine.
These letters serve as a warning shot to the health agencies that if they don’t do as the petition requests, there will be legal action taken. The pressure is most definitely mounting as each of these actions creates another chink in their bureaucratic armor.
Remdesivir in Oklahoma: The Daily Clout legal team sent a letter to Ascension Health Group informing them that they’re on notice to stop using Remdesivir due to the data that shows it’s killing people, along with a request to research therapeutics.
CDC On Notice: Oregon State Senators Kim Thatcher and Dennis Linthicum along with Dr. Henry Healy have officially received a response from the CDC regarding their notification of a demand for a grand jury investigation. The response was negative as expected, but the response triggered a 60-day timeline for the CDC to take substantive action, or the next stage toward a grand jury investigation will advance.
A Demand for Answers: Administrative Judge Alejandro Recarey is a judge in Uruguay. As reported by Rio Times Online, an official complaint was filed to request an injunction of the children’s Covid vaccinations, a request that they are immediately suspended. In response, Judge Recarey ordered that the government health agencies, as well as Pfizer, must appear in by today, Wed July 6 at 9:00 AM and provide answers to the following questions, among others:
Contracts between the Uruguayan government and Pfizer. Included in that must be any information regarding compensation for victims of side effects.
Information about how the vaccine batches were distributed, and what quality control measures are taken.
“Detailed information on the biochemical composition of the vaccine – including whether graphene oxide and nanotechnology components are included”
Evidence that the mRNA they used is harmless.
A definitive statement on if any part of the vaccine, or the vaccine itself is experimental.
Data showing the safety and efficacy of the vaccination.
Information about the average age of “Covid-19 deaths” and how many of those had co-morbidities.
Information about what, if any, studies are being done to investigate an increase of deaths in Uruguay from March 2021.
Scientific evidence that unvaccinated people pose a risk.
Information on connections that exist between the people who are the driving force behind the vaccine campaign, and pharmaceutical companies or NGOs.
Information on how thoroughly alternative therapies against covid-19 have been researched and considered.
All eyes on Latin America!
UPDATE AFTER ETANA HECHT WROTE HER ARTICLE - here is a link to the Uruguayan decree of a halt for the shots for kids under 13:
https://childrenshealthdefense.org/defender/uruguay-covid-vaccine-kids/
Keep praying to the Creator. Psalms are especially powerful.
G-d made me stumble on this photo just before. It’s a great ending:
Here are Etana Hecht’s and Pierre Kory’s full original articles:
