


On Deadly Censorship and Lies, AND THEIR GOALS
When you control the media and suppress all information that goes against your narrative, you can lie all you want. Too many people have no idea of the extent to which this is being perpetrated.

BS”D
This article is extra long, because I’m attempting to show in one space the censorship and lies that we are living through, and why this is being done.
First, the censorship part.
I want to begin to illustrate the foundational point - that we are experiencing extreme and unprecedented censorship in medical and scientific debate, and in media, social media, news, advertising - for a very nefarious purpose - through a fascinating article by Dr. Pierre Kory, a “tzaddik” of a doctor whom I’m personally in contact with. (Tzaddik means a righteous individual, and Dr. Kory has continuously shown himself to care passionately about saving human life, and to put that consideration above his personal career and income.) Dr. Pierre Kory is one of the foremost covid care treatment doctors in the world, and one of the world’s top ICU doctors as well.
Dr. Kory leads us through some instances of heated scientific debate on medical topics which he and Dr. Paul Marek participated in, showing how even hotly contested topics were talked out, and thereby often the truth emerged. This is in complete contrast to the total media and medical establishment blackout on the truth around COVID-19 treatments the last two and a half years. His article is really eye-opening.
When you realize this, you can also understand how much the media and other powers have shaped the beliefs of the population about gender, about family and marriage and having kids…. about G-d, and EVERYTHING around how to live and what is right and good. The influence they’ve had on ALL of us is inestimable, and it’s all towards their goals of population reduction and control over us, which I’ll demonstrate at the end.
After Dr. Kory’s piece, I want to show you yesterday’s New York Times article, which is a great illustration of the misinformation they get away with when censorship is allowed. This is what Dr. Kory is talking about. If you’re an informed person, the lies in the NYT jump out at you so blatantly that it’s simply mind boggling how they can write such stuff.
Here’s Dr. Kory’s article:
The Historic Suppression of Scientific Debate in COVID
Never before in modern history have entire topics in Medicine been actively prevented from discussion in public forums. As a result most of the world only heard one-sided narratives.
By Dr. Pierre Kory MD MPA
I started reading about the definition, history, and legal background of censorship. The entry on Wikipedia (ugh) was quite revealing:
Censorship is the suppression of speech, public communication, or other information. This may be done on the basis that such material is considered objectionable, harmful, or sensitive. Censorship can be conducted by governments, private institutions and other controlling bodies.
But get this, look at the examples of topics that have traditionally been censored:
General censorship occurs for a variety of claimed reasons including national security, to control obscenity, pornography, and hate speech, to protect children or other vulnerable groups, to promote or restrict political or religious views, and to prevent slander and libel.
Note that “scientific opinion” is not on there. Because neither scientific data nor interpretations of that data should ever be considered offensive. You can argue that wrong interpretations of data can be harmful, but debate is how you resolve that, not censorship! Science literally rests on open debate and the sharing of data and exchanging of interpretations amongst not only experts, but the wider public.
Now, also from Wikipedia:
Censorship has been criticized throughout history for being unfair and hindering progress. Censorship is counterproductive as it prevents the censored topic from being discussed. Those who impose censorship must consider what they censor to be true, as individuals believing themselves to be correct would welcome the opportunity to disprove those with opposing views (just ask Steve Kirsch).
But again, science is not on there as a category of discourse to censor. Although history is replete with attempts to censor individuals with scientific views contrary to established orthodoxy, in all the instances I can think of, the person being censored was eventually proven correct!
Yet, in the last 2 years we have undergone a massive censorship of the discussion and sharing of scientific data in public forums. I believe this was the proximate cause of what can now only be viewed as humanitarian catastrophes resulting from 1) the suppression of knowledge of early treatment with effective repurposed drugs and 2) the suppression of data showing the toxicity, lethality, and ineffectiveness of the vaccines.
This period should serve as one of the most damning arguments against censorship.
We were not allowed to openly discuss our data or our interpretations and applications of that scientific data (i.e. scientific opinions) in major media or social media. The journalist Matt Taibbi called me “the ghost of the internet” because whenever I had a scientific discussion with folks who are now dear friends and colleagues, their content and podcasts were de-platformed or demonetized (as in the case of my dear friend Dr. Been), and/or they immediately founds their posted videos of those discussions taken down, like immediately (the speed in which I “disappeared” was astonishingly fast at times). All because we had a scientific discussion where I had shared data and interpretations of that data. I was honored with the opportunity to make my case in front of some truly expert and deep thinkers. Folks who could challenge me, ask questions, express concerns or offer alternative interpretations or hypotheses. I would say that the only problem with those discussions is that the data in support of ivermectin was just so overwhelming. It is a drug with proven efficacy in COVID. Note that conclusion is shared by some of the most highly published doctors in the history of our specialty (the FLCCC) as well as by a group of some of the top evidence-based medicine researchers in the world (Tess Lawrie, Andrew Bryant, Edmund Fordham et al. of EBMc2).
And therein lay the problem. The data could not be debated because any other interpretation than ivermectin being effective was pretty much indefensible in the face of a mountain of repeatedly and almost universally supportive data from myriad sources. So, instead, such discussions were banned from wider public view. Strong move. I think the only thing that saved a good portion of humanity was that individual and organizational websites (like the FLCCC’s, AAPS, c19early.com, and others) were largely secure and not taken down or booted off of hosting servers. But I imagine they could have been.
So, in COVID, Big Pharma and Big Government literally got media companies to shut down debate and discussion on certain topics like HCQ and IVM and vaccine toxicity and ineffectiveness. See YouTube’s community guidelines, which are so absurd, I literally turn purple with rage every time I read it. But it is also sort of comical because they literally put it in writing, right out in the open, plain to see, essentially saying “thou shalt not discuss these medicines on our platform.” And they did it while their efficacy was still being debated. In a global pandemic with thousands dying each day. Safe medicines.
Check it out:
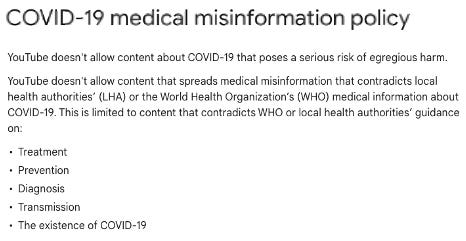
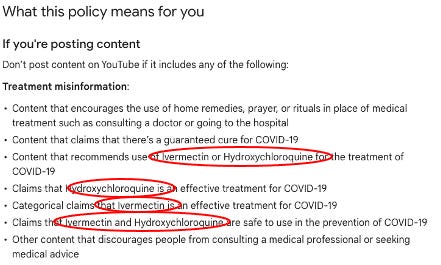
Insane. Crazy town. Clown world. Now, keep in mind that these “guidelines” restricting any discussion of the efficacy, even potential efficacy during a global pandemic, were employed by every major media company in the world with few exceptions, like Trial Site News (although massively impactful, not yet “major media”) and maybe on a few occasions Fox News or some conservative radio hosts.
But all was not lost. Independent podcasters and some radio hosts saved the day, contributing to the dissemination of life-saving information to millions of people in this country and world. Folks like Bret Weinstein, Joe Rogan, John Campbell, Dr. Been, Dr. Mercola, Greg Hunter, Vicki McKenna (hi Vicki!) and countless others. But the print and TV media giants did not have that policy written and made public for all to see (and laugh at). It was under the table, understood by all media that ivermectin should instead only be referred to as a horse dewormer. Not subtle. Alex Berenson’s recent sharing of evidence that the White House was behind his Twitter de-platforming shows how high up the censorship was coming from.
So you literally had the government and Pharma pressuring all the media and social media giants (all of them - Facebook, Linked in, Instagram, Twitter etc) to outlaw, yes, outlaw discussion of even the possibility these medications were effective. Never, ever forget this. Note how YouTube wrote that their guidelines were based on WHO recommendations. Control the top, you control everything beneath it. Read my detailed deep dive uncovering the corruption of ivermectin at the WHO here and here.
Now, one of the reasons Paul Marik was such a famous critical care doctor is that he had long been successful at debunking prevailing orthodoxy supporting standard of care practices in our specialty. He did it via lecturing and debating at national conferences and in publications within medical journals. It was how he and I met, when he congratulated me on an editorial I wrote in a major journal, where I argued against using ultrasound to measure the size of the inferior vena cava to estimate central venous pressure (CVP), largely drawing on the science and rationale he had compiled and published.
Talking to Paul this morning, he told me he is most proud of his work (note he accomplished this feat on his own) in teaching a global generation of critical care doctors that measuring the CVP to estimate the fluid needs of a patient was useless outside of a very narrow set of circumstances like hemorrhage (in those circumstances though, you don’t need the CVP to estimate fluid needs as the patients vitals and clinical presentation will tell you all you need to do.
You have to understand that the CVP was used for decades by critical care doctors in ICU patients who were in states of shock (dangerously low blood pressure). It was the standard of care in ICU’s. Paul did a deep dive into the published literature and especially into the complex physiology of the factors which influence CVP and wrote pretty much the coolest and most impactful paper ever called “Does Central Venous Pressure Predict Fluid Responsiveness?: A Systematic Review of the Literature and the Tale of Seven Mares.” The papers most memorable sentence was “the only study we could find demonstrating the utility of CVP in predicting volume status was performed in seven standing, awake mares undergoing controlled hemorrhage.” Brilliant. Funny.
His paper triggered fierce and I mean, fierce debate in critical care… for years. Reversing established orthodoxy in medicine (and anywhere really) is nearly impossible. But Paul singlehandedly pulled it off with his papers and lectures (helped by a lot of folks like me who followed his work closely). I would argue that today, the obsession with using the CVP to guide fluid resuscitation has largely (but never completely) been abandoned. Wow.
But, again, back then, you could have “debates” on controversial topics, in fact, such topics demanded them! I remember when the United Hospital Fund used to put on this terrific conference in Manhattan where they invited experts in the field to debate “controversies” in critical care (like CVP). Each speaker was given ten minutes and were assigned the pro side or the con side of a topic, but the assigned debaters could not choose the side to argue! After both speakers were heard, the audience voted on which conclusion was based on the more compelling data and argument. I was invited several years in a row and sometimes had to argue the side I was not on intellectually. Which made it even more enlightening an exercise - imagine getting Berenson to have to argue in support of ivermectin? It just might happen that he learns something important. Also, it was a “hard” ten minutes they gave you. So much so, I remember one year I got the whole room laughing because I did not shut up when the big timer hit ten minutes and the big red stoplight turned on, so a close colleague of mine ran up to the podium, put me in a headlock and started to drag me away from the podium as I was still yelling my final points. That was fun. Now, not so much.
More trips down the memory lane of debates. One of the first “corruptions” by Pharma that I experienced in my career was when Eli Lilly invented a national campaign called “Surviving Sepsis” in an attempt to create guidelines supporting optimal care practices. They involved all the professional societies in critical care to participate. Leaders in the field all with a seat at the table.
Yep, you guessed it, it turned out to be cover for their efforts in making a $5,000 harmful drug (Xygris) the standard of care in sepsis. Every single one of those committee members got money. The entire campaign and strategy was developed by a PR firm. Recall that Disinformation tactics were first invented by a PR firm in the 1950’s working for the Tobacco Industry at a time when their products were starting to look bad in the scientific literature.
I would argue that Pharma is the most skilled practitioner of Disinformation amongst all industries. I mean 20 years ago already, the entire country’s critical care doctors gave a very expensive, harmful drug to every septic patient for years based on a manipulated trial with the tiniest of mortality benefits amidst a splashy “public health” campaign concocted by a PR firm working for a pharmaceutical company.
When Xygris was eventually shown to be harmful it was abandoned. But that decision occurred on the back of fierce debates and constant re-analysis and discussion of the accumulating data. Hmm, I wonder when that will happen to Remdesivir? Fun fact: during my fellowship training in pulmonary and critical care, my mentors, Dr. Paul Mayo and Dr. Samual Acquah essentially forbade the use of Xygris at a time when every other fellow in training was using it like water. I never once ordered it for any patient.
But there were other controversial aspects of the sepsis guidelines that Paul was a beast in demolishing at national conferences. He was so good, his take on the data so expert and compelling that his lectures were always packed, like standing room only type packed. For a medical lecture.
The most debated aspect of sepsis treatment (and yes, it was debated repeatedly at national conferences) was called “early goal directed therapy” (EGDT) which required that you resuscitate patients using fluids and vasopressors to a target central venous pressure (CVP) and a target central venous oxygen saturation (SCV02), but to monitor the latter continuously, you had to insert a special catheter into the large neck veins to do it. I will not go into the detailed physiology of those parameters but the need to measure them was nonsense.
I knew it (even as a fellow), my mentors knew it, Paul knew it, yet EGDT was widely adopted across the country and world. The protocol was based on a single center study whose Principal Investigator Manny Rivers held the patent on that catheter (unknown by most at the time). Further, information later came out that the data were manipulated. That information was leaked by a whistleblower who was a fellow of Rivers at the time. The fellow was threatened by the hospital with the ending of his career if he were to continue to speak publicly about it. They even apparently threatened to “kill his kids.”
But the point is, the debates were fierce, in the open, and at conferences and hospital auditoriums across the country and world. They were data driven arguments by experts with decades of scientific inquiry and clinical expertise who reviewed the physiology and published literature. And sometimes led to conflicting interpretations. Yes, we all had biases when interpreting the data (all humans do), but we debated. It was not outlawed to say that SCV02 and IVC were unnecessary. Or to say they were critical. And you were not forced to use all aspects of EGDT in the care of patients back then as they were just “guidelines,” not rigid protocols supported by Federal government funded bonuses in every patient you used it in like we have now with Remdesivir.
Interestingly, widespread EGDT adoption actually showed consistent impacts in reducing mortality, but we knew it was not from the targeting of those parameters but instead just from the early recognition and resuscitation of sepsis. Might even be the one instance in history where a corrupt action by Big Pharma actually led to a benefit in public health. Anyway, eventually studies showed that targeting those parameters versus simply using clinical judgement led to the same outcomes and the practice was abandoned. Paul was right again.
Another aspect of the U.S resuscitation guidelines that Paul was absolutely brilliant in debunking was the decision to target a reduction in lactate as a resuscitation endpoint. This was another fiction like the CVP. Again, almost all of emergency and critical care medicine had been indoctrinated with the physiologic concept that lactate is a marker of hypo-perfusion (reduction in blood flow to organs). Now, in certain, specific clinical instances (ischemic bowel etc), a rise in lactate can reflect hypo-perfusion. But in most septic patients it is simply a marker of illness and stress. It is not harmful, in fact, if anything, lactate is better utilized by organs to maintain function and energy. However, doctors were taught to target lactate as a resuscitation endpoint instead of simply interpreting it as a marker of disease severity.
But, in this instance, that practice and belief was not the result of corruption. No-one as far as I can tell was making money off of dumb doctors and nurses being forced to check lactates repeatedly. It simply stemmed from ignorance and established practice, with leading “experts” (dotards) arrogantly teaching that it was important to target (because they were taught that and did not critically think about it). Paul’s research revealed that targeting lactate was the result of a gross misunderstanding of lactic acid physiology. It was again one of the most masterful papers I have read. He marshaled tons of physiologic knowledge and logically presented the concepts and data which defined the cause and purpose of lactic acid production.
Just like with his teachings on CVP, again you had one man arguing against an entire generation of doctors who believed that reducing lactate was important in the general septic patient. I totally agreed with Paul’s papers and conclusions. Which made my life difficult because I tried in vain to disseminate this knowledge among my trainees, trying to stop what I saw as the pervasive “lacto-bolo reflex” they were all exhibiting. Paul actually invented the term, and it was brilliant: “bolo” refers to a bolus of fluids, and the “reflex” was the ordering of an infusion of a half liter or liter of fluids every time a high lactate was measured.
Lacto-bolo reflexes unfortunately led to what he also brilliantly coined as “salt water drowning,” i.e the receipt of excessive amounts of saline fluids by patients. Every time a doctor or nurse received a report of a high lactate… the doc ordered fluids. Lacto-bolo reflex. What is crazy is that the excess fluid administration that resulted paradoxically worsened kidney function and led to more kidney failure despite the fact the doctors were trying to preserve kidney function with fluid infusions! It was insane and I knew it because of Paul’s research and teaching. I also tried for years to fight the lacto-bolo reflex in my trainees and colleagues with little success except for when I was physically present in the ICU. When I went home for the night though, my fellows and residents all continued with their lacto-bolo reflexes. When the cat’s away the mice will play.
However, in this instance, despite Paul’s papers and lectures on the topic, the unthinkable became true. “Experts” (dotards) eventually established the checking of repeated lactate as a national quality of care standard. Those standards are what hospitals are judged on which affects their reimbursement and accreditation.
So, doctors across the country are now literally mandated to repeatedly check and respond to lactates in septic patients. Again, another example of an orthodoxy based on fiction. Despite all of Pauls efforts in teaching, lecturing, and publishing on the topic, this time, he was unsuccessful in changing orthodoxy. He may have been if his career didn’t end, but History marches on. I would argue that his efforts in singlehandedly trying to reverse orthodoxies unfounded by “the science” led to a widespread respect, admiration, and reverence for the deep knowledge and scientific acumen he consistently displayed. But not so much anymore it seems.
And that is solely because Paul’s final effort in academic medicine was in trying to reverse the fiction that ivermectin was ineffective in COVID. That effort ended his career because for the first time, unrealized by him at the time, instead of fighting ignorant knowledge of physiology, he was poking The Bear, i.e tackling a subject that threatened Big Pharma. In a big, big way. Thus, that effort ended his career. But let’s be specific about that - his former hospital (SENTARA GENERAL IN NORFOLK, VIRGINA) was the one who actually ended his career.
Now, how they ended it is pretty interesting, as my last job was ended in the same way. They did it by using a process that hospitals have long employed when a physician “doesn’t toe the line.” In COVID, Paul was a clinical leader in a major hospital and was employing a highly effective protocol using a combination of repurposed drugs and not using Remdesivir. And he was vocal about it. And he was teaching the doctors in training about the harms of Remdesivir and all of the data supporting “unapproved therapies.” So, they invoked a process called “sham peer review" to get rid of him. What is “sham peer review?”
From a seminal paper on the topic:
In 1986, the United States Congress enacted the Healthcare Quality Improvement Act (HCQIA). which granted immunity to hospitals and reviewers participating in “good faith” peer review of physicians and dentists. These reviews were envisioned to be vehicles by which it could be determined if any actions or recommendations against a physician should become necessary on the measures of incompetence, unprofessional conduct, or behaviors that impact the doctors’ clinical privileges. However, of late, HCQIA has resulted in many unforeseen consequences, not the least of which is the rise of ‘sham peer reviews’ —and the consignment of guiltless, lifesaving, pre-eminent physicians into obscurity.
What is “Sham” Peer Review?
Sham peer review is an adverse action taken in bad faith by a hospital for purposes other than the furtherance of quality health care. It is a process that is disguised to look like legitimate peer review. But sham peer review is not objectively reasonable, precisely because it is not performed to advance the quality of health care (violation of safe harbor provision).
A sham peer review happens when the hospital invents some pretext on which to attack the physician and acts to disguise the adverse action against the targeted physician by conducting a such a review—where the truth and the facts do not matter, because the process is contrived to be rigged, and the outcome is predetermined.
Over the years, sham peer reviews have unfortunately become fairly well-known. Hospitals in the United States have mounted these proceedings for at least four decades to rid themselves of physicians who “get in their way.” Often, they are doctors who don’t ”follow the party line” and whom they consider “disruptive.” Hospital officials are resistant to physicians who bring patient safety or care quality concerns to their attention. Some hospitals retaliate against these whistleblowers, by instigating these sham peer reviews.
How Sham Peer Review works
Hospitals that use sham peer review bring trumped up, fabricated, and thoroughly false charges against the targeted physician. Although no court of law would permit depriving an accused person of files or records needed to defend himself, as it is fundamentally unfair and in violation of due process, hospitals that employ sham peer review frequently refuse to provide records required to the physician under review. Based on these totally erroneous and phony charges the physician’s hospital privileges are summarily suspended. The physician is usually given 14 days to respond in writing to the sham charges. The charges and the physician’s response are then supposedly shared with the Medical Executive Committee (MEC). The physician then meets with the Medical Executive Committee. The physician is usually denied legal representation (which is unlawful), and the meeting takes the form of a Kangaroo court.
And the above, is EXACTLY what happened to Paul. Like.. to the T. Most importantly, he had no rights during the process. No ability to bring a lawyer in to help defend him. No ability to discover the identity of the complainant or exact documentation of the complaint. That is how they can just make things up.
I won’t go into the details because the above explains everything that happened to Paul but his was particularly egregious (mine was short and simple). They generated at least 8 anonymous, invented complaints by other providers, nurses and employees inventing things he said or did and characterizing his behavior as “disruptive.” He had never gotten a single complaint from a patient or colleague in his entire career. They even accused him of malpractice for treating a patient for severe COVID who had tested negative for COVID. I saw the patient’s films and labs, heard his history, and presentation. The guy had COVID, period. Plus, the guy was super sick, on a ventilator, and Paul saved him with his protocol. No small feat for a COVID patient on a ventilator. The patient survived yet the hospital used the case as a mark against him. Insane.
Everything was right out of the sham peer review playbook. And it resulted in the ending of his career.
My “sham peer review” was different given that I was working as an independent contractor running an ICU for a hospital in central Wisconsin. The hospital administration had been asking my partners who hired me to get rid of me as soon as they heard I had been hired, likely due to my public profile (ya think?). My partners refused as we got along great and they deeply appreciated my skills, contributions, COVID expertise and protocols. They told the administration “if he goes, we go.” And this was a hospital with a long track record of difficulty recruiting physicians. Yet, my partners were continually harassed by the administration who kept sending them “hit pieces” they found about me in newspapers and magazines.
Six months later, in November 2021, the Chief Medical Officer of the hospital knew I was not vaccinated and that a mandate was about to start. So he called me and asked if I was going to be vaccinated because he had to plan for contingencies. I asked him for a couple of days to think about it. I decided I would just get a vaccine card instead. Not proud of that plan but I knew the vaccines were built on unconscionable lies. He called me two days later, and I told him I would get vaccinated.
The next morning after my shift, my lead partner called and told me “they didn’t need me anymore.” I asked what happened (I knew they needed me, badly). He explained that I had told some ER patient to not get vaccinated and that their practice believed in vaccination so could not be associated with someone who was not. One catch - I had not been in the ER for two weeks. I defended myself, to no avail. My partner knew I was telling the truth, but I knew he was likely under an ultimatum. He apologized and said, “I am so sorry, but there is a war going on and you are unfortunately a casualty of that.” We said pleasant goodbyes and wished each other well. Pretty quick sham peer review because I was not an employee so they had the right to cancel my contract at anytime. Done. Gone.
So, as you can see from the above, COVID is not our first rodeo battling ignorance and corruption in Medicine. But we battled with debate using data, published literature, and deep knowledge of physiology. Now, no more.
Steve Kirsch has been offering 1-2 million dollars for anyone in academia or the agencies to participate in a public or even privately recorded, moderated debate of the evidence to support vaccine safety and efficacy. No-one took him up on it.
An organization in Kansas City asked me, Peter McCullough and two other experts to participate in a debate with the clinical leaders at KU. They refused to show. Their table sat empty on the stage while we debated the public statements they had made with a local TV program instead. They literally told the TV presenter that “we do not debate in public forums, only in journal clubs amongst fellow doctors.” Note he said this on TV then went on to support their policies citing what we know are corrupt and easily disprovable evidence-free narratives. What a farce.
Just as sad as the above is that Paul had long been invited every year by a medical education organization to lecture to anesthesiologists as he was a perennial favorite lecturer. This past year, he gave a masterful lecture on the data supporting the use of ivermectin in COVID. Soon after, he was told that he will never again be invited to give lectures.
He also gave the same lecture to the Anesthesia Department at Mass General (Harvard). The evaluations by attendees all complained that his lecture was full of mis-information. He will never be invited back.
Twitter, which describes itself as a “public square” has de-platformed many of my colleagues (multiple times) for sharing newly emerging data supporting the efficacy of ivermectin. Hey Juan Chamie, how many times have you been Twitterwhacked? One of life’s greatest mysteries (slight overstatement) is how I am still alive on Twitter, although to be accurate, I am only half-alive as they severely shadow ban me on that platform.
I guess we just have to accept the fact that two new commandments have come down from the mountaintop:
Thou shalt not share favorable ivermectin data in any public media sphere
Thou shalt not present analyses of the scientific data supporting ivermectin in lectures to physicians
The world has gone mad.
••••
That’s the end of Dr. Kory’s article from August 30 (link to original at end), but he had an interesting follow up piece yesterday about three ivermectin semi-debates that he remembered after he published the article. I’ll just quote the first. He wrote:
This one was a doozy. It occurred at the last hospital I worked at. I had been using high-dose ivermectin in ICU patients there for months when suddenly the world’s most deadliest propaganda PR campaign against ivermectin was launched in August of 2021, you know the “horse dewormer” one (I will lay out in chronological and structural detail how they conducted that campaign in my next post).
Anyway, it was a smallish hospital (200+ beds with like 32 ICU beds) where the head Infectious Disease doctor was initially neutral on ivermectin but we became colleagues, I found him open-minded, he asked appropriate questions and was receptive to receiving and digesting the data I had compiled. I began to share the mountains of data supporting ivermectin in COVID. He was shocked at how much data there was and he also instantly fell in love, like I did, with the c19early.com site, a site which many researchers have relied upon in COVID as it is the most comprehensive and sophisticated compilation and analysis of the data supporting dozens (yes dozens) of effective therapies in the treatment and prevention of COVID. Although anonymous, I just want to say thank you to that group for the absolute superlative work you all have done. Their anonymity tells you that this isn’t their first rodeo in publishing “inconvenient science.” I wish they had warned us in the FLCCC. Or not. :)
Anyway, he ended up reviewing a fair amount of the trials data and was fully supportive of my use in the ICU. He even got the pharmacy to order more to support my clinical practice. It was incredible. So far so good.
However, he related to me that he was doing so over the objections of the head Infectious Disease Pharmacist… who was very, very much against the use of ivermectin in COVID. Simple reason: his diet consisted solely of edicts from captured high-impact medical journals and health agencies.
Anyway, the doc outranked him so my patients’ access to ivermectin was secure… until he was suddenly re-assigned to a different hospital in the system just prior to the start of Pharma’s PR campaign against ivermectin in August 2021. Uh oh. Not good.
Note that Pharmas’ opening salvo in the biggest battle of their War on Ivermectin (Title of my upcoming book) was when they got the CDC to issue a fraudulent memo which warned all U.S doctors and pharmacists that ivermectin poisonings were on the rise. The memo also reminded the nations doctors that the FDA had not “authorized” the drug for use in COVID (umm.. they don’t have to authorize it as my readers well know). That my friends, is just one of the “tells” that the CDC was trying to manipulate doctor behavior on behalf of their masters (Pharma). Anyway, that memo also went to every state Pharmacy Board and thus it landed in the inbox of every licensed Pharmacist of every state across the land within 24 hours. Whoa.
I am sure he was inspired by this move because he immediately decided to take down Dr. Kory and his penchant for treating patients with one of history’s safest medicines. Within days I was visited in my office above the ICU by the Chief Medical Officer who told me that the “P & T” (Pharmacy and Therapeutics) Committee was holding a meeting in a few days to decide whether ivermectin would continue to be stocked and available in the hospital pharmacy for use in COVID. Uh oh again.
Knowing that I was literally one of the world experts on the clinical use of ivermectin in COVID-19, he invited me to present to the Committee in order to inform any decision on ivermectin that they would make. I immediately knew where this was heading but, if you know anything about me by now, I don’t go down without a fight. So I accepted.
He told me that the Infectious Disease Pharmacist felt it should be removed (of course he did) and that if I wanted to continue to use it, I could present my argument for why it should remain on the hospital formulary. Note that these decisions are effectively what the P & T Committee in every hospital makes, i.e. they decide on what therapies should be made available and for what conditions depending on their efficacy, risks and especially costs.
Game on. Couple of days later, the meeting was held on Zoom, and I cleverly pretended I was having a computer issue so I was able to ask that he go first while I supposedly “worked it out” (tactics baby, I wanted him to go first, to see what kind of butter knives he was bringing to this gun fight so that I could counter optimally). I also knew lives depended on it.
This was his approach: he presented the two negative trials that had been published in high impact journals at the time, which I knew he was going to do, but the rest of his slides consisted simply of the logo of an important health agency and their individual recommendation against ivermectin. First slide: WHO: against use outside of a clinical trial. Infectious Disease Society of America: against use outside of a clinical trial. And it went on and on, slide after slide of him reading the same recommendation over and over. European Medicines Agency, American Medical Association, Society of Emergency Medicine etc. You get it. Not a bad move actually.
So then I went, first explaining the glaring issues with those two trials (and they were glaring), and then reminding the group that the highest form of medical evidence is a meta-analysis (i.e when you combine data from all existing trials to estimate the average level of benefit). Then I essentially presented the entire evidence base: meta-analyses of the RCT’s, the OCT’s, plus the health ministry data out of Mexico City, Peru, Brazil, Uttar Pradesh, Argentina etc. It was pretty convincing to me but whatever.
The highlight (or lowlight) of the meeting was when, just after I finished, I asked “Are there any questions?” There was a fairly long pause (Del’s “NIH pause”) until a Committee Member asked “Dr. Kory, why are your data and the recommendations of all the agencies so discordant?”
I also paused, took in a deep sigh and said, “there is really only one answer to that, and that is that me and my group have no conflicts of interest around the use of ivermectin.” Boom. Drop mic.
Not.
They thanked me for my time, and I left the zoom so they could have their discussion and then hold their vote. Two days later the CMO again came to find me personally, sat down in my office and informed me that the hospital had decided that they were removing ivermectin from the formulary and that I would no longer be able to prescribe it to patients.
Pierre 0, Clown World, 1.
••••
Now I want to show you a striking example of how a highly respected newspaper which shapes public opinion (the New York Times) can twist the truth so blatantly. They get away with this because they and their friends do their best to make sure that opposing information is never presented to the mainstream.
What the side of censorship has done is to blame and vilify those who immediately promoted effective treatment for covid, and whose treatment they mocked and suppressed, as they said “there is no cure for covid”, thereby killing hundreds of thousands and purposefully hyping the fear as high as possible.
But now that their “own”, harmful “early treatment” has come out (Paxlovid), they take full credit for contributing to the “lessening of covid anxiety” among those very people whose fears they themselves stoked.
Unbelievably, they blame “Trump and some Republicans” for creating “covid anxiety” even as they write in the very same article that those who identify as “very liberal” took extra covid precautions in order to not be mistaken for conservatives (who were known to not take covid as seriously.)
Recently, as the truth is seeping out and they are attempting to cover themselves, the side of censorship simultaneously manages to praise the covid vaccines’ “effectiveness” and talk about “all the lives it saves” while blaming Trump for rolling it out quickly “over the FDA’s objections.”
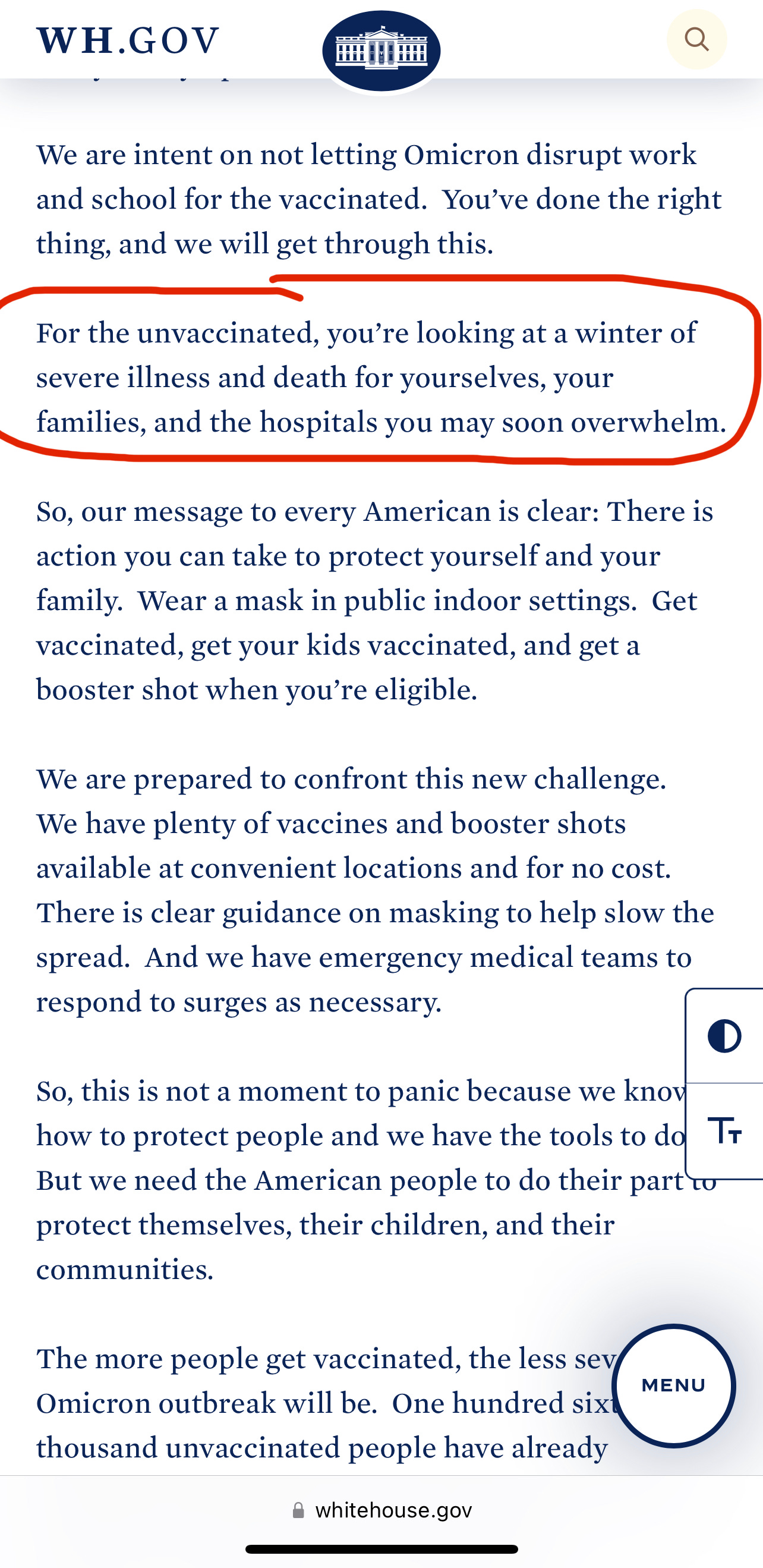
Strangely, the current administration is credited for lowering covid anxiety. 😂 Surely nobody forgot that Biden is the one who, last fall and again this summer, gravely warned of a coming “winter of severe illness and death”?
They are twisting themselves into pretzels, doing mental gymnastics.
Here are excerpts from yesterday’s NYT article. I have bolded the parts that jumped out at me as most significant.
Good morning. Americans on the left end of the political spectrum have become less anxious about Covid.
By David Leonhardt
Shrinking partisan gaps
Almost six months ago, when my Morning colleagues and I released our last poll about Covid, the deep anxiety among Americans identifying as “very liberal” was one of the main findings.
Forty-seven percent of very liberal adults said that they believed Covid presented a “great risk” to their own personal health and well-being. That was a significantly larger share than among conservatives, moderates or even liberals who stopped short of calling themselves very liberal. Particularly striking was the level of concern among liberals under age 45, even though the virus’s worst effects have been concentrated among older people.
Oh, now they admit that young people really don’t have what to fear? Don’t I recall scary articles in MSM trying to get across the message that people of any age should be afraid of dying of covid?
I understand why attitudes about the virus vary so sharply by ideology. Our country is polarized on most high-profile issues today. In the case of Covid, Donald Trump and some other Republicans exacerbated the divide by making a series of false statements that downplayed the threat or misrepresented the vaccines.
I’m getting confused over here. Is the “other side” to blame for minimizing or for maximizing the risks of covid? For yes vaccine or no vaccine?
To many liberals, taking Covid seriously — more seriously, at times, than the scientific evidence justified — became an expression of identity and solidarity. As one progressive activist tweeted last year, “The inconvenience of having to wear a mask is more than worth it to have people not think I’m a conservative.”
So now they admit that this wasn’t about science; it was a cult.
This morning, we’re releasing the results of our latest Covid poll (which, like the earlier ones, was conducted by Morning Consult). This time, one of the central findings is how much attitudes have changed since the spring. Americans are less worried about the virus today — and driving that decline is the receding level of anxiety among the very liberal, including many younger adults.
The share of the very liberal who say the virus presents a great risk to their own personal health has fallen to 34 percent.
A growing number of very liberal Americans have decided that it’s time to treat Covid as an unpleasant but manageable part of life, much as many other Americans — as well as people in other countries — decided months ago.
Shame on you, NYT. After killing and destroying so many, you now see which way the wind is blowing and you’re trying to jump on the bandwagon.
What explains the change? In part, it’s probably a reflection of changing reality. Drugs like Paxlovid and Evusheld are now widely available, reducing the risks for vulnerable people.
Hydroxychloroquine and Ivermectin, zinc, D and C, are super effective at saving lives, but the NYT has worked hard to make sure most people think otherwise. https://www.nytimes.com/2022/03/30/health/covid-ivermectin-hospitalization.html
But psychology seems to play a role too. After all, many aspects of the pandemic have not changed in the past six months. Both then and now, vaccines provided excellent protection against severe illness; the risks of hospitalization for children and most adults under 50 were minuscule; and the vaccines reduced the chances of long Covid.
Excellent protection against severe illness? Exactly the opposite:

All of which suggests that the decreasing anxiety among liberals also stems partly from the passage of time. Trump has not been president for more than 18 months. In his place is a Democrat pushing progressive policies on climate change, health care and student loans — and also encouraging Americans not to let Covid fears dominate their lives.
Really? It’s a good thing we have the records. Here’s a press briefing on December 17, 2021 by the White House COVID-19 Response Team:
The NYT author could not resist a parting pitch for the killer shots:
The federal government is likely to approve the next generation of booster shots — designed to be even more effective against the latest variants — in coming days. Within a week or two, these new shots will probably be available to Americans 12 and older.
Wait, I thought the ones we already have are extremely effective? 😂
On a not-so-funny note, the new shots are VERY worrisome, as they are BRAND new - they have not had ANY HUMAN SAFETY TESTING AT ALL. Believe it or not, they were tested on a total of 8 mice, who had a wildly uneven antibody response, and actually went on to develop covid.
A useful rule of thumb is that anybody who has not yet received a shot in 2022 should consider doing so in coming weeks. As Dr. Ashish Jha, the White House Covid coordinator, told me yesterday: “It’s really important, especially if you’re at elevated risk, but really for anyone. If you have not had a booster this year, it’s critical that you go and get one.”
Which way is it? Did the NYT just admit young people are at minuscule risk? If so, why is it “critical”they go and get a booster?
Severe Covid illness continues to be heavily concentrated among people over 65, especially those who are unvaccinated or not current on their booster shots.
So, he still concludes with the well-trodden lie, which contradicts all the actual infection and death data separated out by vaccine status which we have publicly available, (from the U.K. for example), which shows that vaccination greatly increases the risk of illness and death, and each shot makes things worse.
There is so much more evidence; it’s mountainous. Some of it: the testimony of funeral workers or embalmers in NY, Alabama, England and Australia (see Australia here: https://www.warroomforum.com/threads/funeral-director-sounds-the-alarm….32292/) and the testimony of the brave healthcare professionals who are speaking up, all showing greatly increased illness and death among vaccinated individuals. Not only do they do worse with the covid infection and get other infections they weren’t previously susceptible to, but they are tragically succumbing to rapidly growing cancers and also just dying suddenly- as courageous scientists warned would happen. If you are new to this, watch the recordings of my events on Macabim.org and RofimInternational.org, and see my previous articles, plus the substack writings of Dr. Pierre Kory, Dr. Jessica Rose, Professor Mark Crispin Miller, Igor Chudov, Steve Kirsch, and many more. For example:

So now, what is the goal of all these lies? Is it just about money, or is there a very evil, malevolent force here, which seeks to harm, not just as an accidental product of profit-seeking, but as a goal in itself?
Yes, there absolutely is. You probably saw my August 30 article, “Who is Behind the Global Murder and Mayhem”, and you may have seen my previous writing about Amalek, the force in every generation seeking to plant doubt about the existence of G-d and His power and His ability to sustain all His creations, and to wage was against Him - to actually attempt to supplant Him.
THIS is the diabolical population reduction agenda we now face, under the cover of “saving our planet” and “conserving our natural resources.”
My Rabbi pointed out to me that unbelievably, Nimrod, who built the Tower of Bavel to fight against G-d, also claimed “climate change”!
Nimrod (who lived a few hundred years after the Flood), made up the story that every 1,656 years (the span between Creation and the Flood), the “skies collapse”, and that’s what caused the Flood.
The Tower was meant to be the first of three pillars they planned, which would support the sky and prevent it from caving in again.
(G-d told us in the Torah why He brought the Flood - because humanity had become hopelessly corrupted. The sins that tipped the scale were stealing and homosexuality - in particular, they wrote marriage contracts (legalized marriage) between man-and-man and between man-and-beast.
But instead of learning their lesson from the wicked ones who had preceded them and been destroyed, Nimrod invented a “natural” explanation for the Flood and invented a story to motivate the people to build a huge Tower.
Some people intended the Tower to be for holding up the sky, while others intended it to be for purposes of fighting G-d.
In the end, each group was punished severely by G-d, commensurate with their intentions.
G-d always sends the perfect information my way to include in the articles, so I just got this illustration of the evil Nimrod-like Amalek’s plans. Remember, theirs is a cult of scarcity, because they don’t believe G-d has enough for everyone.
WEF AI to Decide what Industries to Liquidate to "Stop Economic Growth"
By Igor Chudov
A brand new video from the World Economic Forum’s agenda article! The agenda is to stop growth and decide what industries to shut down.
Some very juicy quotes from the video (with timestamps)
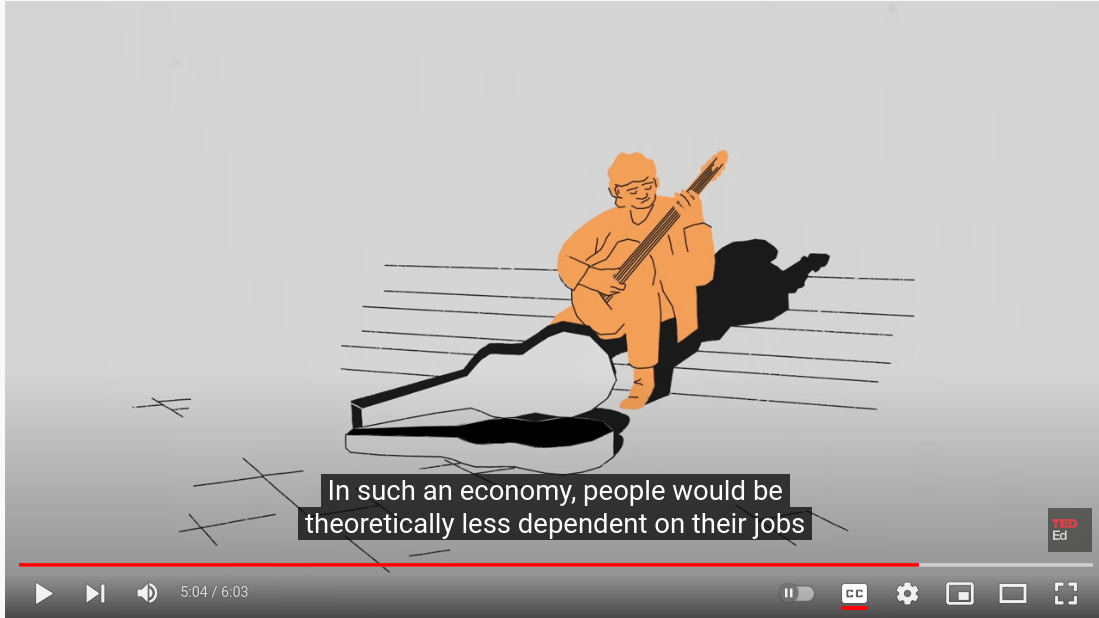
4.23: Some economists think the solution is to reengineer our economies completely. They make the case that what we should really be doing is weaning ourselves from the addiction to growth and shifting to a post-growth economy (later defined as liquidation of various industries — I.C)
Instead of growing, WEF wants us to focus on what we “really need” (according to WEF)
4:46 things like renewable energy, healthcare, and public transportation. To do that, economists think that rich countries should do something like guarantee living wages.
They are talking about unearned “universal basic income” because the next cut shows a sad-looking lonely person spending a day not working. It promises that people will not be needing jobs to “earn their living or get healthcare”:
What is the goal? To scale down production of things deemed less necessary! (sic)

WEF asks if we could “do away with entire industries”, showing an anxious, sweaty man worried about his industry being shut down:

How would we decide what is unnecessary, asks the voice prompter. How would we resolve our disagreements? How to make these decisions?
The answer is, says WEF, is that we need to enlist help from AI systems, in order to answer the questions such as which industries to do away with.

WEF loves AI!
See pieces of the World Economic Forum’s article:

Source: https://www.weforum.org/agenda/2022/09/can-the-economy-grow-for-ever-teded/
Here is the next piece of evidence:
(I need to caution that the site I’m about to quote from, the Covid Blog, has other articles which are anti-Jewish and which I find strongly objectionable and not grounded in reality. However, the following seems to be totally legitimate, as it correlates perfectly with information I already have, such as the independently verified goals of the UN and their subsidiary, the WHO.)
Depopulation Agenda: Planned Parenthood’s documented blueprint for destroying humanity comes to fruition over last 50 years, culminating with COVID-19
Excerpts:
Billionaires can only buy so much with their money. There are only so many toys and travel destinations in the world. Power is the ultimate goal for these types. They yearn control, the power to administer every move, every thought, and every goal of humanity. The World Economic Forum (WEF), founded and run by Klaus Schwab, made clear that by 2030, humanity will “own nothing and be happy.”
All the usual suspects (Facebook, Google, Bill Gates, PayPal, etc.) are listed as partners of the WEF, along with Johnson & Johnson, AstraZeneca, Pfizer and Moderna.
The United States officially launched its depopulation blueprint in 1969. It has come to nearly 90% fruition in 2021 after hitting some roadblocks in the 1980s. But the talks about depopulation among those in power commenced in the 1930s and progressed from there. Keep these stats in mind as you read this article.
The average American adult woman (up to age 35) had 3.58 kids in 1960(Baby Boomers).
76% of black American babies were born to married mom and dad in 1965.
97% of white babies were born to married mom and dad in 1965
72% of all American adults were married in 1960.
The provisional number of births in the U.S. was 3,605,201 in 2020. That is the lowest number of births in the United States since 1979, according to the Centers for Disease Control. 2020 also had the lowest fertility rate since the government started tracking births in 1902. And don’t blame the so-called “pandemic.” Birth rates have been steadily declining since 2007, when 4.3 million babies were born in the United States. Total fertility rates have been below replacement – meaning the number of births necessary for a generation to replace itself – since 1971.
The depopulation agenda is deliberate and documented. This article chronicles the depopulation journey from 1916 to today.
1916-1942: The race-based beginnings of U.S. population control
Planned Parenthood and its founder, Margaret Sanger, are the progenitors of all modern population control agendas in the United States. It’s important to note that Planned Parenthood receives a vast majority of its funding from the federal government, thus is essentially a government organization. The first “birth control clinic” opened on October 16, 1916 in the Brownsville section of Brooklyn, New York. One website described Brownsville, at that time, as “a down-trodden part of New York City where the ‘inferior races’ and ‘human weeds’ lived; immigrant southern Europeans, Slavs, Latins and Jews.” Today Brownsville is predominately Black.
Sanger began publishing the magazine Birth Control Review in 1917. Though Sanger was always careful about the language she used in public speeches, her eugenics goals were blatant and obvious. The July 1922 issue of Birth Control Review, stated the following as a founding goal:
“Sterilization of the insane and feeble-minded and the encouragement of this operation upon those afflicted with inherited or transmissible diseases, with the understanding that sterilization does not deprive the individual of his or her sex expression, but merely renders him incapable of producing children.”
Sanger founded The American Birth Control League in 1921, according to the Encyclopedia of Women’s History in America. Its mission statement not only reiterated Sanger’s goal of eugenics, but racially-targeted eugenics.
THE AMERICAN BIRTH CONTROL LEAGUE. Its Aim: To promote eugenic birth selection throughout the United States so that there may be more well‑born and fewer ill‑born children ― a stronger, healthier, more intelligent race … and in order that those who are physically and mentally unsound may use birth control to have fewer or no children” Birth Control Review, Volume XVI, Number 12 (December 1932), page 319.
Sanger launched her “Negro Project” in 1939. You can read more about that here. But essentially the goal was to stop Black babies from being born at all in the United States. The American Birth Control League changed its name to the Planned Parenthood Federation of America in 1942.
1942-1969: Planned Parenthood hastens destruction of nuclear family
Sanger continued expanding Planned Parenthood and connecting with eugenicists globally and domestically. She established the International Planned Parenthood Federation in 1952. The organization won several victories in courts and on administrative levels in the 1950s and 1960s. The Food and Drug Administration approved the first birth control pill – Enovid-10 – on May 9, 1960. The U.S. Supreme Court struck down all bans on birth control pills for married couples in the 1965 case Griswold vs. Connecticut. Sanger died one year after the decision. But the organization was left in “good” hands.
Further on:
The damage was done to Black Americans. The situation continually worsened until it reached abyss levels in 2021. But eugenicists weren’t satisfied. They now had the blueprint to population control and manipulation – destroy the nuclear family. White families had been unaffected by all of the happenings of the 1960s. A new strategy was necessary, as the same tactics used to hasten Black family self-destruction wouldn’t work on white families.
Birth control pills were mainstream among white women by the late 1960s. That alone slowed births quite a bit. But Planned Parenthood and its partners had loftier goals for global population control.
1969: the official start to modern global depopulation
Mainstream media “fact-checkers” (e.g. Snopes and Politifact) say that Bill Gates, Sr. never worked for Planned Parenthood and dismiss the whole idea as “conspiracy theory.” Planned Parenthood websites have scrubbed all remnants of Gates Sr. working for them. Unfortunately for mainstream media, Bill Jr. spilled the beans in a May 9, 2003 PBS interview. Like eugenicist father, like eugenicist son. Gates Jr. told Bill Moyers:
When I was growing up, my parents were always involved in various volunteer things. My dad was head of Planned Parenthood. And it was very controversial to be involved with that. And so it’s fascinating. At the dinner table my parents are very good at sharing the things that they were doing. And almost treating us like adults, talking about that.
The full PBS transcript is here. Bill Gates Jr. was born in 1955. Thus he was “growing up” in the 1960s and early 1970s. That is the time frame that Gates, Sr. headed Planned Parenthood, likely after Sanger died. His visions extended far beyond Sanger’s black genocide goals. The organization and its partners forged ahead with its new, larger visions.
The Jaffe Memo
Frederick S. Jaffe was the Vice President of Planned Parenthood in 1969. He was also Executive Director of Planned Parenthood’s Center for Family Planning Program Development. He wrote a memorandum in response to a request from Bernard Berelson, who at the time was President of the Rockefeller-founded Population Council. The March 11, 1969 letter became known as the Jaffe Memo.
The 9-page document is a fascinating read into the minds of eugenicists and depopulation advocates. But it is page 9 that is essentially the blueprint for everything that has happened since 1969 related to American families, social norms, sexuality and depopulation. A table outlines “Proposed Measures to Reduce Fertility by universality or Selectivity of Impact in the U.S.”
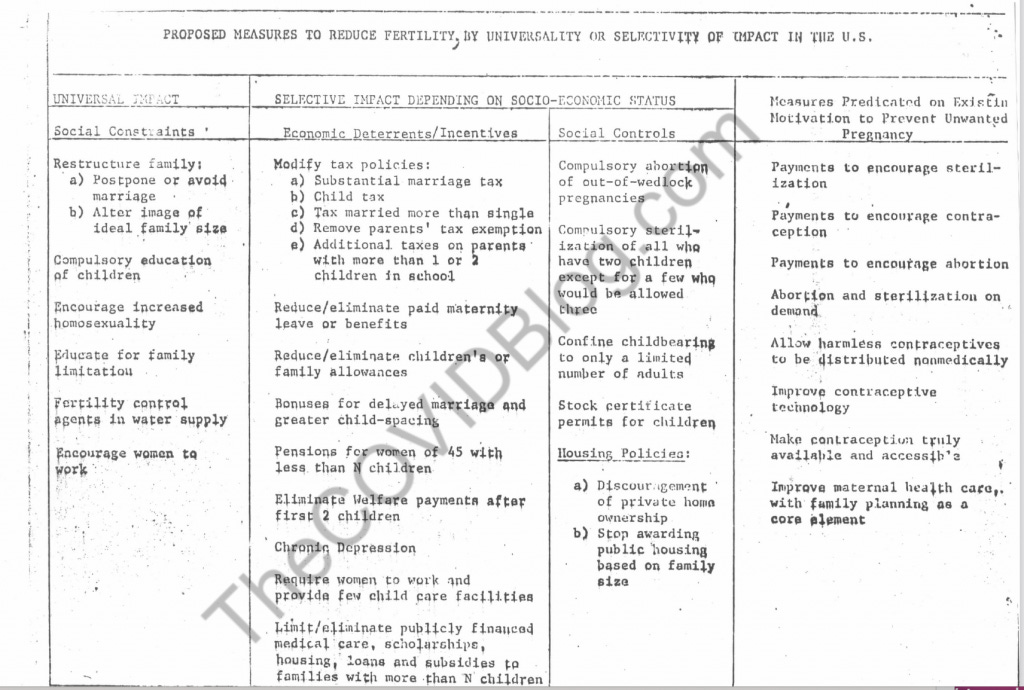
The full document is here if the screenshot is hard to read. The left-hand column outlines Universal Impact measures for Social Constraints.
Restructure family – alter image of ideal family and avoid/postpone marriage
Compulsory [public] education for children
Encourage increased homosexuality
Fertility control agents in water supply
Encourage women to work
Payments to encourage self-sterilization, contraception and abortions are also proposed in the document. It also discourages private home ownership.
Planned Parenthood’s Center for Family Planning Program Development broke away from the organization in 1974 and became the non-profit subsidiary Guttmacher Institute. It was named after Dr. Alan Guttmacher, an OB-GYN and former Vice President of the American Eugenics Society (now called the Society for Biodemography and Social Biology). The Guttmacher Institute officially split from Planned Parenthood in 2007. Jaffe headed the Guttmacher Institute until his death in 1978.
Of course mainstream media “fact-checkers” have done amazing word gymnastics trying to discredit the Jaffe Memo as “conspiracy theory.” But again, read it for yourself and continue reading this article.
Legal abortions and executing the homosexual agenda
Planned Parenthood and the Population Council were and are very influential. They also have bottomless government funds. The organizations immediately went to work executing the Jaffe Memo in real-life.
The homosexual agenda is necessary to destroy nuclear families, destroy the natural, common sense fact of man and woman; and cull overall birth numbers. Obviously homosexual “couples” cannot procreate without weird science. The more homosexuality, the less procreation.
Abortion and Planned Parenthood victories in 1970s
The Family Planning Services and Public Research Act was signed into law by President Richard Nixon in 1970. Known more broadly as Title X, the bill guarantees federal funding “dedicated to providing individuals with comprehensive family planning and related preventive health services.” Since 2010, the Title X program received about $300 million in taxpayer funds per year, every year.
New York was the first state to legalize abortionin 1970. Planned Parenthood opened its first legal abortion clinic in Syracuse, New York that year. But federal law still prohibited the practice. The U.S. Supreme Court broadened its ruling in the aforementioned Griswold case in 1972. The Court, in Eisenstadt vs. Baird, extended legal contraception to unmarried couples as well – essentially everyone. Back-alley, illegal abortion clinics operated in many cities in the 1960s. Of course Roe vs. Wade was decided in 1973, legalizing abortions in all 50 states.
Normalizing homosexuality
Abortion and birth control were now fully legal across the U.S., just three years after the Jaffe Memo. Now it was time to fully implement homosexual culture as legal, protected and sacred. The American Psychiatric Association updated its Diagnostic and Statistical Manual (DSM-II) in 1973. It changed homosexuality from a mental disorder to a “sexual orientation disturbance” and a “normal sexual variant.” The International Gay Association (now ILGA) was founded in 1978. Homosexual culture was well on its way to becoming a protected, mainstream class of people as it was integral in the overall population control agenda.
80’s backlash to homosexuality, while women work
National and global psy-ops need a coordinated mainstream media to work. Television shows and movies in the 1970s and 1980s depicted women as workers and career people.
The agenda was working, in that women now worked just as much as men. And it had the desired effect. Fertility rates were slashed in half in a matter of 20 years. The average American woman had 3.58 kids in 1960. That number dropped to 1.77 kids by 1979. Out-of-wedlock births spiked dramatically among Black Americans, from about 20% in 1960 to 55% in 1980. But most importantly to the eugenicists, the plan was working, albeit more slowly, for White Americans too. Out-of-wedlock white births rose from 3% in 1960 to about 12% in 1980.
Women were officially workers first, instead of mothers and wives. Most women – 60% – used birth control pills or some other contraception by 1988.
The depopulation agenda, in accordance with the Jaffe blueprint, is essentially a mission accomplished by 2019. Birth rates continually plummeted to their current all-time lows. The nuclear family is nearing extinction. Nearly 40% of all American babies were born to a single mom in 2018, according to the CDC. That’s up from 12% in 1980. About 70% of black babies were born to single moms in 2018. And 30% of white babies were born to single moms in 2018, up from 3% in 1960 and 12% in 1980. Birth control and abortion are normalized. Men are now called women (“trans”). Those who fail to play along with these word games are cancelled “bigots.”
Let’s recap. The 1969 Jaffe Memo appears to be the blueprint for everything happening in 2021. Fertility rates are at all-time lows in 2020. Nuclear family is nearly extinct in the United States. In 1949, 79% of U.S. households had a married couple. Today, that number is 48%. Groundwater is contaminated with gender-bending chemicals. Homosexual culture (“LGBT”) is now the most protected, sacred people in America because they are not procreating. This agenda also ensures that the nuclear family continues its path to extinction.
COVID-19 is the final chapter in the depopulation agenda for both the United States and world.
Links to other articles quoted:

Please share.
And please pray to the Creator of Heaven and Earth to save His world.
BS”D
You are completely correct about Canada. I wrote about it a while ago, but someone told me yesterday that it now progressed to an even more horrifying level. I need to find the documentation. Meanwhile, here are the previous articles where I tried to expose Canada’s euthanasia laws: https://truth613.substack.com/p/the-holocaust-and-our-current-situation and https://truth613.substack.com/p/the-government-is-not-your-friend
BS”D
Brucha, it is almost Erev Yom Hakippurim. Your literary efforts are so major and magnificent, that you are not only an Eishes Chaiyel, you are also a Tzaddick in our time. You have ennobled our world, in the manner of Deborah, of Yehudit, and of Esther.
If you deem it possible and useful, please expose the latest chillul Ha’Shem, to wit: it has become lawful, or is about to become so, in Canada to legalize the recommendation of euthanasia to sick or suicidal patients by hospital personnel or governmental authorities, according to reports sent to me. This will achieve financial gains for eugenicists and government officials. This is a step ahead of the “mere” legalization of assisted suicide as seen in Europe, and Washington State and Oregon reportedly. To advise and/ or to counsel suicide is obscene, in my opinion, and violative of all moral codes, and indicative of the abysmal depths to which government has fallen.