


Part 2: The Great Cholesterol and Saturated Fat Scam /The Deadly Dangers of Statins
If cholesterol is a nutrient essential to life and health, to building new cells and to repairing damage caused by inflammation, what do you think the outcome of blocking cholesterol would be?

BS”D
As we showed in Part 1, the entire foundation upon which statin treatment is built reflects a terribly faulty understanding of not only the huge importance of cholesterol to every cell in the body, but of the true causes of heart disease itself.

Here in Part 2 I will focus on the severe harms caused by statin treatment.
My first real dive into the utter corruption and falsehood in the manipulated statin trial “results,” the disingenuous medical journal articles, and the resulting statin recommendations by teams of bribed “experts” was when I read Overdosed America: The Broken Promise of American Medicine by Dr. John Abramson MD. It remains one of my favorite books, and I strongly urge everyone to obtain a copy. Dr. Abramson thoroughly demonstrates the criminal ludicrousness of statin prescription (as well as other for-profit medical frauds.) You can find his book on Amazon.

In addition to the subtle, commonly unrecognized and very widespread adverse effects of statin use, (for example, it has been found that 100% of statin users show mild cognitive decline, if a sensitive enough test is used to detect it) there are the exceedingly tragic but less common top-of-the-bell-curve reactions, such as rhabdomyolysis, a potentially fatal muscle-wasting side effect. You can even google it:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5853001/
I wonder whether the elderly patients who are routinely given statins are given true informed consent about the possibility of rhabdomyolysis and other potential severe harms, such as organ failure, diabetes, ALS, Parkinson’s, amnesia, dementia, aggression, depression, and hearing loss? Shouldn’t everyone have a real chance to weigh the imaginary “benefits” against the documented harms and choose for themselves? Instead, patients are propagandized to believe that the only thing standing between them and a fatal heart attack is the “lifesaving” statin pill, which could hardly be further from the truth.
Remember from Part 1 that lowered cholesterol does NOT correspond to lowered risk of death, or of heart disease, as multiple studies confirm.
For example, a 56 month randomized study of 9,423 adults (inconveniently) found that for every 30 points their cholesterol dropped, their risk of death increased by 22 percent.
From the paper on the NIH site:
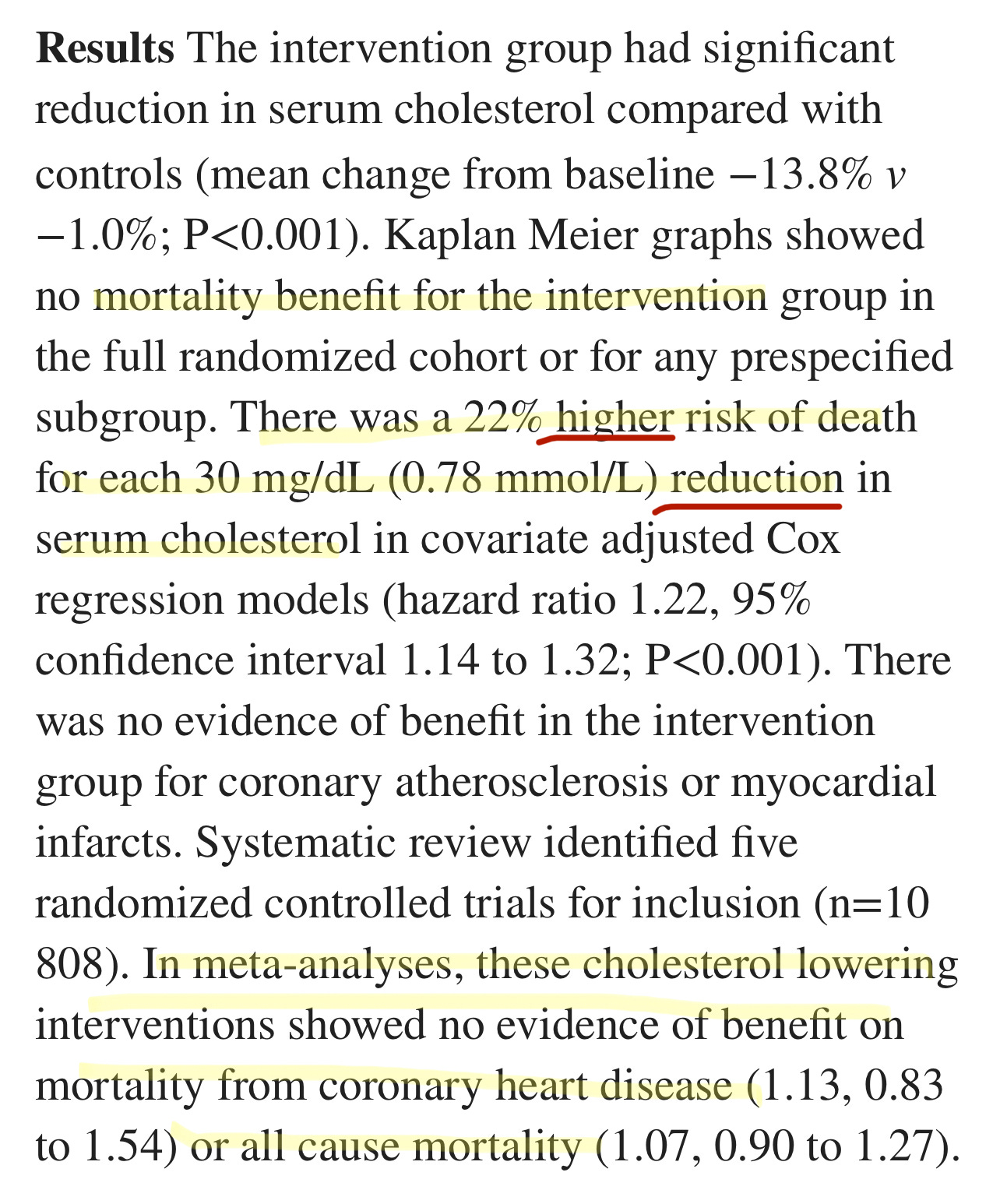
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4836695/
A 1986 study in the Lancet concluded:
During 10 years of follow-up from Dec 1, 1986, to Oct 1, 1996, a total of 642 participants died. Each 1 mmol/L increase in total cholesterol corresponded to a 15% decrease in mortality (risk ratio 0–85 [95% Cl 0·79–0·91]).
Regarding heart disease risk: this study, this study, this study, this review, this review, and this review.
This is simply astonishing. For what possible “benefits” are patients being subjected to the life-ruining effects of statins? Surely, the benefits are only financial - to the drug manufacturers and to the prescribers.
Tragically, rather than any sort of informed consent, patients not only have statins aggressively pushed on them, as A Midwestern Doctor details below, but are gaslit when they complain of adverse effects they’re experiencing. They’re told “statins can’t cause that.”
Well, yes, they can.
Here are parts of AMD’s excellent review of statin harms.
By A Midwestern Doctor - link to original article at end:
Statin Injuries
My primary issue with the statins is not the fact we waste billions each year on a useless therapy (approximately 25 billion dollars per year in America alone). Rather, it’s the fact that they have a very high rate of injury. For example, the existing studies find between a 5-30% rate of injuries, and Dr. Malhotra, having gone through all the existing evidence, estimates that 20% of statin users are injured by them.
Likewise, statins are well known for having a high percentage of patients discontinue the drugs due to their side effects (e.g., one large study found 44.7% of older adults discontinue the drugs within a year of starting them, while another large study of adults of all ages found 47% discontinued within a year).
Statins in turn, are linked to a large number of complications that have been well-characterized (e.g., mechanistically) and described throughout the medical literature.1, 2, 3, 4, 5, 6
One group of side effects are those perceived by the patient (which often make them want to stop using the medications). These include:
Psychiatric and neurologic issues such as depression, confusion, aggression, and memory loss1, 2, 3, 4, 5, 6, 7, 8, 9
Severe irritability1
Sleep Issues2
Sudden (sensorineural) hearing loss1
Gastrointestinal distress1
The other group are those not overtly noticed by the patient. These include:
ALS-like conditions and other central motor disorders (e.g., Parkinson’s disease and cerebellar ataxia)1, 2, 3, 4, 5
Lupus-like syndrome1
Interstitial cystitis1
Polymyalgia rheumatica1
Renal failure1
Cognition is highly dependent upon cholesterol. For example, one study found that minor cognitive impairment could be detected in 100% of statin users if sufficiently sensitive testing was done (which again illustrates how minor injuries are more common than severe ones). Likewise, a variety of more severe adverse effects on cognition are also observed such as amnesia, forgetfulness, confusion, disorientation, and increased senility.
Their patient’s rapid descent into dementia after a statin is started is much too often written off by their doctor as senile brain changes or beginning Alzheimer's when the real culprit is their statin drug.
Note: one of the sadder side effects we have frequently observed from the COVID-19 vaccines has been a rapid cognitive decline in the elderly (who cannot often advocate for themselves). When this happens, like statin damage, it is always assumed to be due to “their age” and ignored.
In addition to cognitive impairment, numerous studies have found a significant association between low or lowered cholesterol levels and violence. Likewise, statin dementia is often characterized by aggression.
One of the most concerning side effects of statins is their tendency to cause ALS (a truly horrible rare disease—curiously also seen in association with the COVID-19 vaccines). This correlation is further supported by many reports of statin ALS improving once the statin is stopped.
Unfortunately, while statin cognitive decline frequently improves when the statin is stopped, in many cases, it instead persists.
From the moment I first encountered statin patients, I quickly noticed that they would report either numbness in their body, muscle weakness and pain, or impaired cognition, which began after they started the statin and resolved once they stopped using it. Remarkably, we also noticed that whenever they (or we) pointed this out to their doctor, the doctor would become extremely hostile, and then insist that the statin could not be causing the symptom (e.g., “because in all their years of practice, they had never had a patient who was injured by a statin”) and that even if it was harming them, the patient needed to stay on it because otherwise they would get a heart attack and die.
In turn, as the years went by, I saw increasingly elaborate excuses being created to protect the statins from an ever-increasing awareness of their dangers. For example, I lost count of how many doctors I knew who cited this 2016 study when patients stated they had been injured:
The nocebo effect, the inverse of the placebo effect, is a well-established phenomenon that is under-appreciated in cardiovascular medicine. It refers to adverse events, usually purely subjective, that result from expectations of harm from a drug, placebo, other therapeutic intervention or a nonmedical situation. These expectations can be driven by many factors including the informed consent form in a clinical trial, warnings about adverse effects communicated by clinicians when prescribing a drug, and information in the media about the dangers of certain treatments.
The nocebo effect is the best explanation for the high rate of muscle and other symptoms attributed to statins in observational studies and clinical practice, but not in randomized controlled trials, where muscle symptoms, and rates of discontinuation due to any adverse event, are generally similar in the statin and placebo groups. Statin-intolerant patients usually tolerate statins under double-blind conditions, indicating that the intolerance has little if any pharmacological basis. Known techniques for minimizing the nocebo effect can be applied to the prevention and management of statin intolerance.
Which, when translated into plain English means that the only reason people believe statins injured them is because they were tricked into imagining the injury, so the best solution is to tell them the symptoms are in their head. What I found remarkable about this study was that the doctors who cited it never considered that the nocebo effect could not apply as their patients were not aware things like muscle pain were associated with statins until they experienced them (and then looked up what was happening) or that the discrepancy in the observed rate of adverse events could also be explained by the fact the randomized controlled trials are always funded by the pharmaceutical industry and hence consistently cover up injuries that occur there.
Similarly, the thing that finally made me realize how impressive the marketing for these drugs had been was the recurring battle I would have with relatives. In each case, I would take them off a statin and provide a strong argument with data supporting why they should not be on the drug. At some point later, they would go to their doctor and inform them that their relative (me), who was a doctor, had taken them off the statin.
Their doctor (often a cardiologist), in turn, would tell my relative I was incredibly ignorant, insist they knew the data much better than I did, say I was endangering my relative’s health, and promptly restart the statin, to which my relative dutifully complied. In many cases, I would provide the cardiologist with literature supporting my argument. In each case, they would make an excuse not to read it while simultaneously asserting that they knew all the data and that I, not being a cardiologist, was unqualified to have an opinion on this subject. This made me appreciate just how challenging a situation patients (without access to the resources my relatives had) were in.
If you take this story and replace “statin” with COVID-19 vaccines, you will see it is essentially what everyone has experienced over the last three years with the vaccines. I suspect this is because, before the COVID-19 vaccines, statins were one of the most profitable medical franchises and, thus amongst the medications most aggressively pushed on patients.
Note: two adverse event reporting systems exist for adverse reactions to pharmaceuticals, MedWatch and FAERS. Like VAERS, they suffer from severe underreporting (it is estimated only 1-10% of adverse events are reported to them). The author in the next section was able to find hundreds to thousands of reports for many of the statin injuries in MedWatch that matched what he had personally observed. However, despite these reports existing, nothing has been done with them, and there is almost no knowledge within the medical community that these adverse events exist.
The Statin Damage Crisis
Throughout this publication, I have tried to make the point that less severe reactions to a toxin are much more common than severe ones. Because of this, if you see a cluster of severe reactions, it indicates that far more, less severe reactions are occurring as well (which is how after learning of a few people in my circle dying suddenly from the COVID vaccines, I was able to correctly predict the scale of the non-fatal injuries that would hit America).
Likewise, if you see a large number of less severe reactions to a pharmaceutical (e.g., the statin-induced muscle and nerve damage), you can predict far more severe injuries are lurking in the background. As the longer list of adverse events I shared above demonstrates, this unfortunately is true for statins. In the next two sections, I will quote one of the best books I have found on this subject:
“Many statin victims say that abruptly, almost in the blink of an eye, they have become old people.”
Duane Graveline MD was started on a statin and soon after developed global amnesia (which is really scary). He decided to stop the statin and recovered.
When I suggested, on the basis of my 23 years as a family doctor, that perhaps my new medicine was the cause of my amnesia, the neurologist replied, almost scoffingly, that "Statins do not do that." He and many other physicians and pharmacists were adamant that this does not occur.”
Eventually, he was persuaded to try again.
The year passed uneventfully and soon it was time for my next astronaut physical. NASA doctors joined the chorus I had come to expect from physicians and pharmacists during the preceding year, that statin drugs did not do this and at their bidding I reluctantly restarted Lipitor at one-half the previous dose. Six weeks later I again descended into the black pit of amnesia, this time for twelve hours and with a retrograde loss of memory back to my high school days.
Later he discovered:
Perhaps stockholder loyalty explains why Pfizer management knew over a decade ago, during the first human use trial of Lipitor, of the cognitive impact to come when Lipitor was released to the public. Of their 2,503 patients tested with Lipitor, seven experienced transient global amnesia attacks and four others experienced other forms of severe memory disturbances, for a total of 11 cases out of 2,503 test patients. This is a ratio of 4.4 cases of severe cognitive loss to result from every 1000 patients that took the drug. Not one word of warning of this was transmitted to the thousands of physicians who soon would be dispensing the drug.
Because of this and other debilitating long-term complications (e.g., previously an extremely fit individual, he developed chronic exhaustion), Graveline became an expert on statin injuries and, in 2014, wrote The Statin Damage Crisis. Many of the points he raised there explain why statins are so dangerous, but unfortunately, are virtually unknown within the medical field.
Statins Marketing
One of the consistent patterns I’ve observed within medicine is that once a drug is identified that can “beneficially” change a number, medical practice guidelines will gradually shift to prioritizing treating that number and before long, rationals will be created that require more and more of the population to be subject to that regimen. In the case of statins, prior to their discovery, it was difficult to reliably lower cholesterol, but once they hit the market, research rapidly emerged stating that cholesterol was more and more dangerous and, hence that more and more people needed to be on statins.
BW: Case in point: In the 1970’s, a cholesterol level of 300 was considered perfectly fine, whereas now, a 2018 American Heart Association paper recommends a cholesterol level of about 150. Money talks.
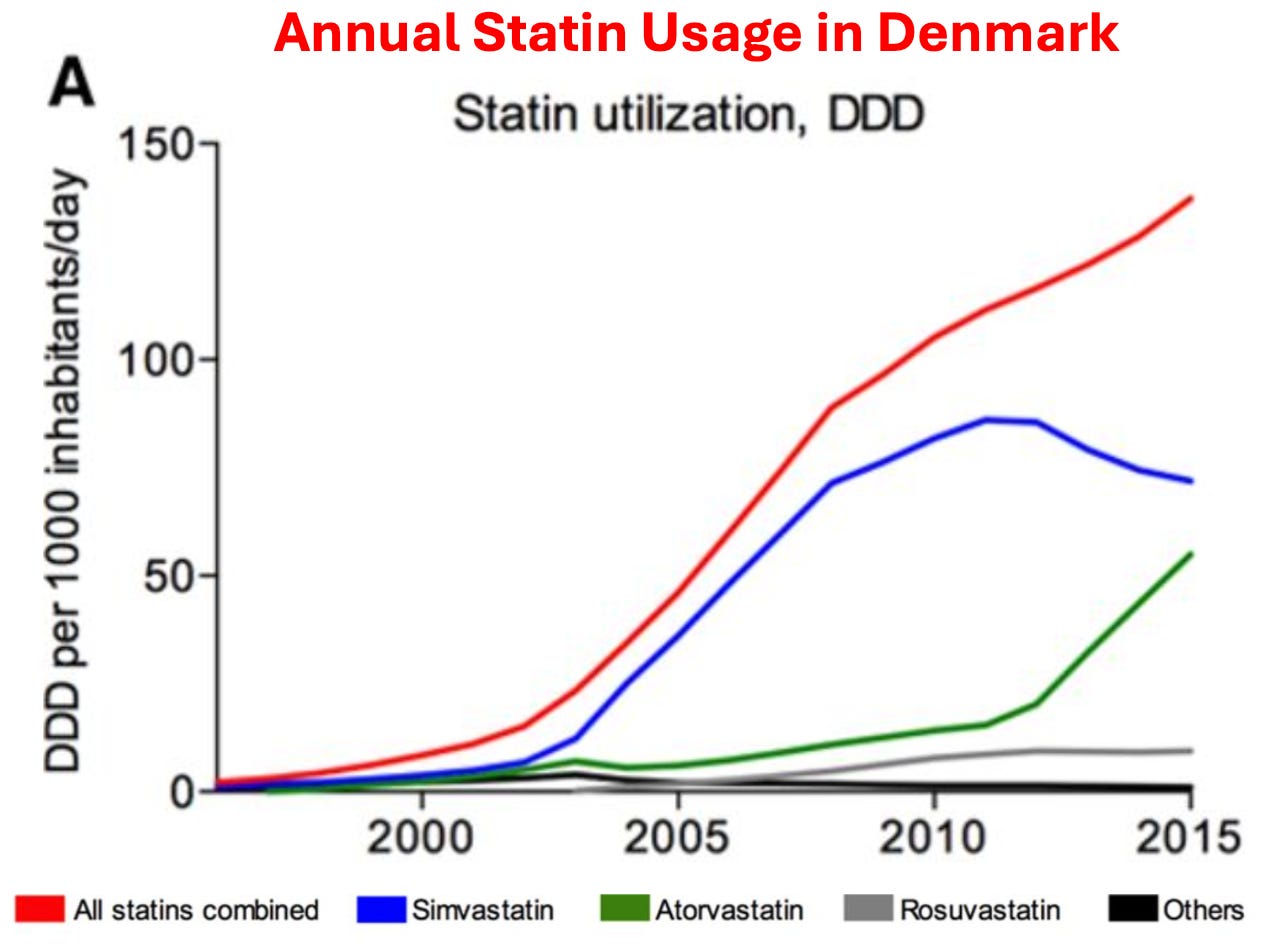
As you would expect, similar increases also occurred within the USA. For example, in 2008-2009, 12% of Americans over 40 reported taking a statin, whereas in 2018-2019, that had increased to 35% of Americans.
Given how much these drugs are used, it then raises a simple question—how much benefit do they produce?
As it turns out, this is a remarkably difficult question to answer as the published studies use a variety of confusing metrics to obfuscate their data (which means that the published statin trials almost certainly inflate the benefits of statin therapy), and more importantly, virtually all of the data on statin therapy is kept by a private research collaboration which consistently publishes glowing reviews of statins (and attacks anyone who claims otherwise) but simultaneously refuses to release their data to outside researchers, which has led to those researchers attempting to get this missing data from the drug regulators.
Note: as you might have guessed, that collaboration takes a lot of money from the pharmaceutical industry.
Nonetheless, when independent researchers looked at the published trials (which almost certainly inflated the benefit of statin therapy) they found that taking a statin daily for approximately 5 years resulted in you living, on average, 3-4 days longer. Sadder still, large trials have found this minuscule “benefit” is only seen in men. In short, most of the benefit from statins is from creative ways to rearrange data and causes of death, not any actual benefit.
BW: Even if the 3-4 days of extra life among men were actually true, which, as AMD notes, is difficult to tell because of the lack of data transparency, the minuscule benefit would NOT be a result of lowering needed cholesterol in the body, but of the anti-inflammatory effect of the statin. This anti-inflammatory effect can be obtained in much safer and more effective ways with a more healthful diet and/or natural products.
In circumstances like these where an unsafe and ineffective but highly lucrative drug must be sold, the next step is typically to pay everyone off to promote it. For example, to quote Chapter 7 of Doctoring Data:
The National Cholesterol Education Programme (NCEP) has been tasked by the National Institutes of Health to develop guidelines [everyone uses] for treating cholesterol levels. Excluding the chair (who was by law prohibited from having financial conflicts of interest), the other 8 members on average were on the payroll of 6 statin manufacturers.
In 2004, NCEP reviewed 5 large statin trials and recommended: “Aggressive LDL lowering for high-risk patients [primary prevention] with lifestyle changes and statins.”
In 2005 a Canadian division of the Cochrane Collaboration [who were not paid off] reviewed 5 large statin trials (3 were the same as NCEP’s, while the other 2 had also reached a positive conclusion for statin therapy). That assessment instead concluded: “Statins have not been shown to provide an overall health benefit in primary prevention trials.”
Likewise, the American College of Cardiology made a calculator to determine your risk of developing a heart attack or stroke in the next ten years based on your age, blood pressure, cholesterol level, and smoking status. In turn, I’ve lost track of how many doctors I saw proudly punch their patient's numbers into it and then inform them that they were at high risk of a stroke or heart attack and urgently needed to start a statin. Given that almost everyone ended up being “high risk” I was not surprised to learn that in 2016, Kaiser completed an extensive study which determined this calculator overestimated the rate of these events by 600%. Sadly, that has not at all deterred the use of this calculator (e.g., medical students are still tested on it for their board examinations).
Note: one of the most unfair things about statins is that the healthcare system decided they are “essential” for your health, so doctors who don’t push them are financially penalized, and likewise patients who don’t take them are as well (e.g., through life insurance premiums).
So, despite the overwhelming evidence against their use, many physicians believe so deeply in the “profound” benefits of statins that they do things like periodically advocating for statins to be added to the drinking water supply.
In tandem, a cancel culture has been created where anyone who challenges the use of statins is immediately labeled as a “statin denier,” accused of being a mass murderer, and effectively canceled. Recently, one of those dissidents, Dr. Aseem Malhotra, a British cardiologist who has also spoken out against the COVID vaccines, went on Joe Rogan where he discussed that dirty industry and the remarkable parallels between how statins and the COVID vaccines were pushed on the world.
Note: one of the most remarkable facts Aseem shared was that the previously mentioned statin collaboration (which militantly insists less than 1% of statin users experience side effects) also created a test one could utilize to determine if one was genetically at risk for a statin injury—and in their marketing for the test said 29% of all statin users were likely to experience side effects (which they then removed once attention was brought to it).
In addition to doctors being forced to follow these guidelines, patients often are too. Doctors often retaliate against patients who do not take statins (similar to how unvaccinated patients were denied essential medical care during COVID-19). Employers sometimes require cholesterol numbers to meet a certain threshold for employment (although they never did anything on the scale of the COVID-19 vaccine mandates placed on workers around America). Similarly, life insurance policies often penalize those with "unsafe" cholesterol numbers.
Please click A Midwestern Doctor’s original article link below for even more information:
I hope that you will share this critical information with loved ones, so that they may perhaps be saved from their ignorant doctors’ clutches.
BW: To help me continue my work, you may make a one-time gift here: https://ko-fi.com/truth613
Thank you so much for this article! I did not know cognition is dependent on cholesterol, and many other things mentioned here. I learned in 1991 that I could take a drug, alter the number in my body, and still have the condition. It had to do with an excruciating dislocated clavicle injury which no one could diagnose and a sed rate of 90, which I was told was 3x the norm. After 1mo. my sed rate was 30, and still I was in horrible pain. So, I was later told I had connective joint tissue disease for which I required meds for life. I rejected that idea as the pain was in 1 spot only and consistently awful. I finally, after 18 months, found someone who correctly diagnosed my clavicle was out of the socket. So many years later when I was told my cholesterol was high and statin was recommended, I didn’t go for it. The part I still don’t understand is the mechanism by which the numbers get altered and reflected in the bloodwork.
I was at a small convention and a cardiologist was talking about the medication pathway he put all his patients on... statins were #1. Another charlatan.